 Avraham Rachamim Chaim Sofer Flyer |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
‘People Are Dying’: Battling Coronavirus Inside a N.Y.C. Hospital | NYT NewsThe New York Times 26March2020
Scenes of “catastrophe” as New York hospitals battle coronavirusCBS This Morning 27March2020 Scale of New York’s coronavirus devastation ‘difficult’ for outsiders to understandSky News Australia 18April2020 The scale of the COVID-19 pandemic is “very difficult for people to understand if they’ve not seen it,” especially in densely populated places like New York, according to physician Dr Qanta Ahmed. The deathtoll from the novel coronavirus has risen above 13,000 in New York, even though the fatality rates have begun to plateau according to the state’s governor Andrew Cuomo. Ms Ahmed told Sky News host Rowan Dean “we are seeing that this disease ravages people who are normally of very good constitutional health” and did not have pre-existing heart conditions or diabetes which makes people more vulnerable to the virus. The former sleep disorder specialist said her hospital on Long Island was four times its normal capacity with infected patients and there are “more critically ill people on respirators than the entire state of Israel, so the scale is incomprehensible even to those of us who are normally there”. Obesity and the population density have also been proven as major contributors in the spread of the virus. With 42 per cent of the population classified as obese, “I am very fearful for the progress of the coronavirus pandemic here in the US,” she said. 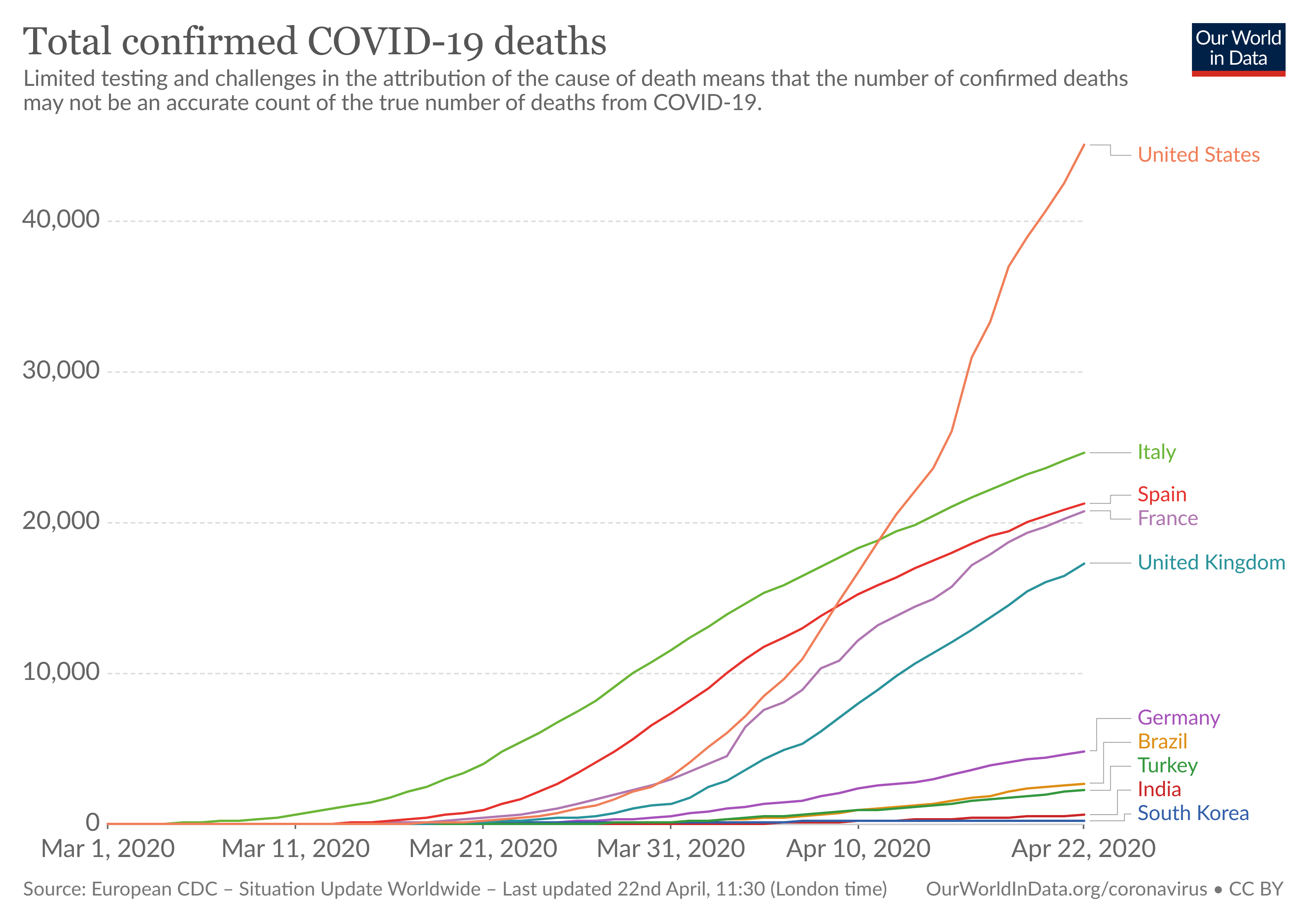 Total Confirmed deaths covid-19 March2020 – 22April2020 by Country https://ourworldindata.org/grapher/total-deaths-covid-19?year=2020-04-12&time=2020-03-01..&country=BRA+FRA+DEU+IND+ITA+KOR+ESP+TUR+GBR+USA 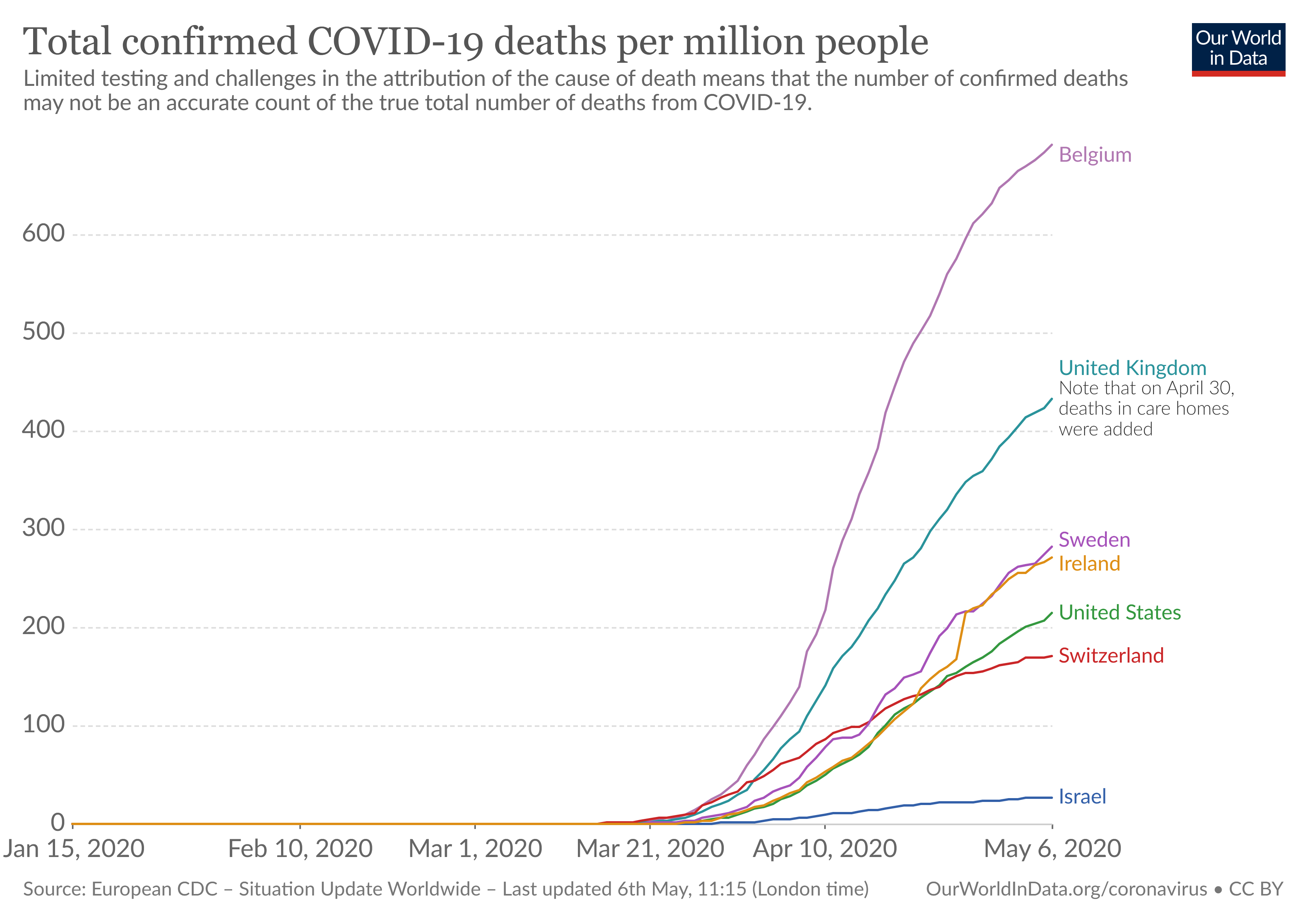 Total confirmed COVID-19 deaths per million people Jan-Apr 2020 country=ISR+BEL+GBR+USA+CHE+SWE+IRL https://ourworldindata.org/grapher/total-covid-deaths-per-million?tab=chart&year=2020-05-06&time=2020-01-15..&country=BEL+IRL+ISR+SWE+CHE+GBR+USA
Flying from NY to Israel during coronavirusPhotographer Shahar Azran decided to fly from NY to Israel. How was the process? How is isolation maintained? What are feelings in NY?Yoni Kempinski, 28May2020 http://www.israelnationalnews.com/News/News.aspx/281008 Photographer Shahar Azran flew from NY to IsraelArutz Sheva TV 27May2020 Arutz Sheva spoke to photographer Shahar Azran, who recently flew to Israel from New York amid coronavirus restrictions. He described the procedure of the flight, how he maintains social distancing now that he is in Israel, and the atmosphere in New York amid the outbreak of the virus. “The city is empty,” he said. “I can’t imagine people going back to the theater in the next 6 months […] We have no idea what’s going to happen. I think New York will be affected more than any other place in the US.” He also predicted that the coronavirus will lead to greater amounts of people moving to Israel. He said that, between the way Israel is perceived as dealing with the crisis and the health insurance issues in the US, “I think more people will think about Aliyah, and it’s a great opportunity for Israel to invest in those great people. “Many people want to move to Israel, now we have to give them a greater inventive to come.” |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
 Number Of Seniors Tapping Social Security Plummets As “Excess Deaths” Spike During Pandemicby Tyler Durden The rate of seniors collecting Social Security benefits has plunged to the lowest level in a decade, which Bloomberg suggests may be due to the disproportionate number of COVID-19 deaths among the elderly. According to the Social Security Administration, the number of people who took retirement benefits rose by just 900,000 to 46.4 million in March, the smallest year-over-year gain since April 2009. 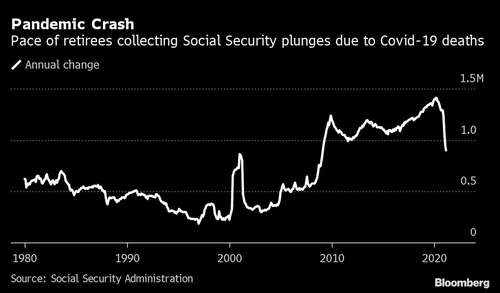 Pace of retirees collecting Social Security plunges due to Covid-19 deaths More via Bloomberg:
According to the CDC, there were 660,200 excess deaths from all causes between January 26, 2020 and February 27, 2021, mostly associated with COVID. 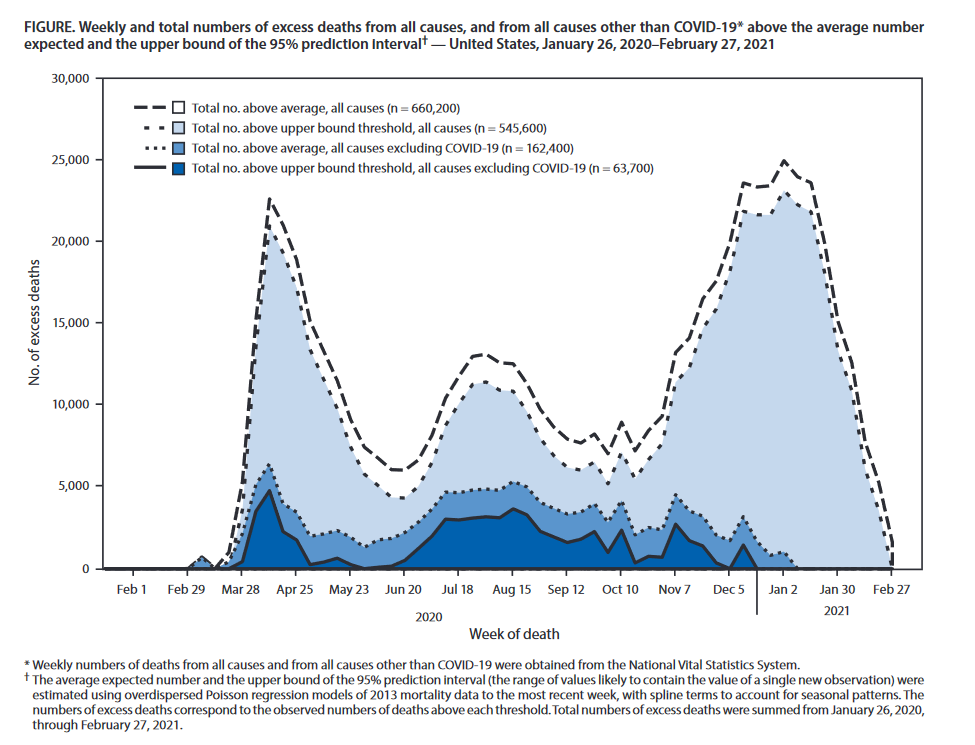 US excess deaths-1-2020 to 2-2021 Bloomberg notes that other factors ‘can’ have an impact on Social Security numbers – for example, “In the early 2000s, the bump in beneficiaries was likely tied to the Senior Citizens’ Freedom to Work Act signed into law in April 2000,” which reduced penalties for beneficiaries who continued to work. That said, there’s nothing of the sort going on which could explain the current dropoff. Life expectancy in the United State plunged by a full year in the first half of 2020 – the biggest drop since WWII – to 77.8 years from 78.8 in 2019 according to the National Center for Health Statistics. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
Ron Paul: How Texas Killed COVIDby Tyler Durden 25May2021 – https://www.zerohedge.com/covid-19/ron-paul-how-texas-killed-covid< Authored by Ron Paul via The Ron Paul Institute for Peace & Prosperity, In March, Governor Greg Abbott announced that Texas would open for business 100 percent without a statewide mask mandate.
The pro-lockdown “experts” were shocked. If a state as big as Texas joined Florida and succeeded in thumbing its nose at “the science” – which told us that for the first time in history healthy people should be forced to stay in their houses and wear oxygen-restricting face masks – then the lockdown narrative would begin falling apart. President Biden famously attacked the decision as “Neanderthal thinking.” Texas Democratic Party Chairman Gilberto Hinojosa warned that, with this order, Abbott would “kill Texans.” Incoming CDC Director Rochelle Walensky tearfully told us about her feelings of “impending doom.” When the poster child for Covid lockdowns Dr. Fauci was asked several weeks later why cases and deaths continued to evaporate in Texas, he answered simply, “I’m not sure.” That moment may have been a look at the man behind the proverbial curtain, who projected his power so confidently until confronted with reality. Now a new study appearing as a National Bureau of Economic Research working paper, highlighted recently in Reason Magazine, has found “no evidence that the reopening affected the rate of new COVID-19 cases in the five-week period following the reopening. …State-level COVID-19 mortality rates were unaffected by the March 10 reopening.” In other words, not only did the doom and gloom predicted by the lockdown fanatics fail to materialize, but the steady, seasonal downward trend of the virus toward extinction continued regardless of government action. As we have repeated for a year on the Liberty Report, the virus was going to virus regardless of anything we did about it. And Texas proved it. However, some very important questions remain to be answered as the Covid panic across the United States is finally starting to recede.
Though Greg Abbott deserves much criticism for shutting Texas down, his re-opening decree effectively ended Covid tyranny across the country. We are thankful for that. Now we must resolve to never let this happen again. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
BREAKING: American Doctors Address COVID-19 Misinformation. Hydroxychloroquine Works!!PatriotDude 27July2020 The Covid Con Game and End GameDr. Lee Merritt, an Orthopedic Surgeon in Onawa, Iowa, is interviewed by Jeff Dornik and delivers an amazingly comprehensive overview of the motives behind the Covid-pandemic theater. First, she shows that there is no real pandemic and that the public-health practices being mandated are scientifically absurd. Then she reasons that, if obscene profits were the only motive for this crime, it would not be necessary to put so many exotic and toxic components into the vaccines. A simpler product could be sold at the same price with a greater profit margin. Therefore, there must be some additional purpose for the vaccines. She makes a compelling case that the end game is nothing less than human enslavement and massive depopulation – both of which are long-held ideals of those who direct the pharmaceutical cartel. 2021 April 21 – Source: Freedom One-on-One |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
The Zelenko protocolhttps://faculty.utrgv.edu/eleftherios.gkioulekas/zelenko/ZelenkoProtocol.pdf
content related to a treatment protocol that has been proposed by Dr. Vladimir Zelenko for the SARS-CoV-2 virus, using hydroxychloroquine, zinc sulfate, and azithtromycin. Dr. Zelenko has recently created his own website crowdprotocol.com to facilitate medical research using crowd-sourced medical data from frontline primary care physicians from all around the world. He has also co-authored and submitted his first paper for publication. See www.thezelenkoprotocol.com for a press release. The website c19study.com is tracking research studies of hydroxychloroquine. A recent white paper by Dr. Simone Gold has documented the safety profile of hydroxychloroquine. Dr. Harvey Risch, from the Yale School of Public Health (and more importantly, a Caltech alumnus), has also published a peer reviewed paper documenting that the aggregate of all research studies to date support the efficacy of the Zelenko protocol, when administered at the early stages of the disease. In doing so, he was criticized by Yale colleagues and wrote a very strong response explaining the fundamentals of the mechanism by which some studies have been used to confound, mislead, and manipulate. The Eastern Virginia Medical School maintains an interesting website with current information for medical practitioners. They recommend an interesting MATH+ treatment protocol for hospitalized patients. They also recommend a quercetin protocol both for prophylaxis and at-home treatment for all patients, but do not recommend hydroxychloroquine protocol, as of June 2020. Both quercetin and hydroxychloroquine are zinc ionophores, however hydroxychloroquine has additional mechanisms of action. Note that Dr. Zelenko recommendsthat the hydroxychloroquine protocol should be prescribed only to at-risk patients, identified as such via specific risk stratification criteria, and recommends the quercetin protocol for low-risk patients. The graph below (retrieved from c19study.com) compares demographically normalized cumulative death curves between nations where the government endorsed using the Zelenko protocol and nations that have opted to discourage its use.
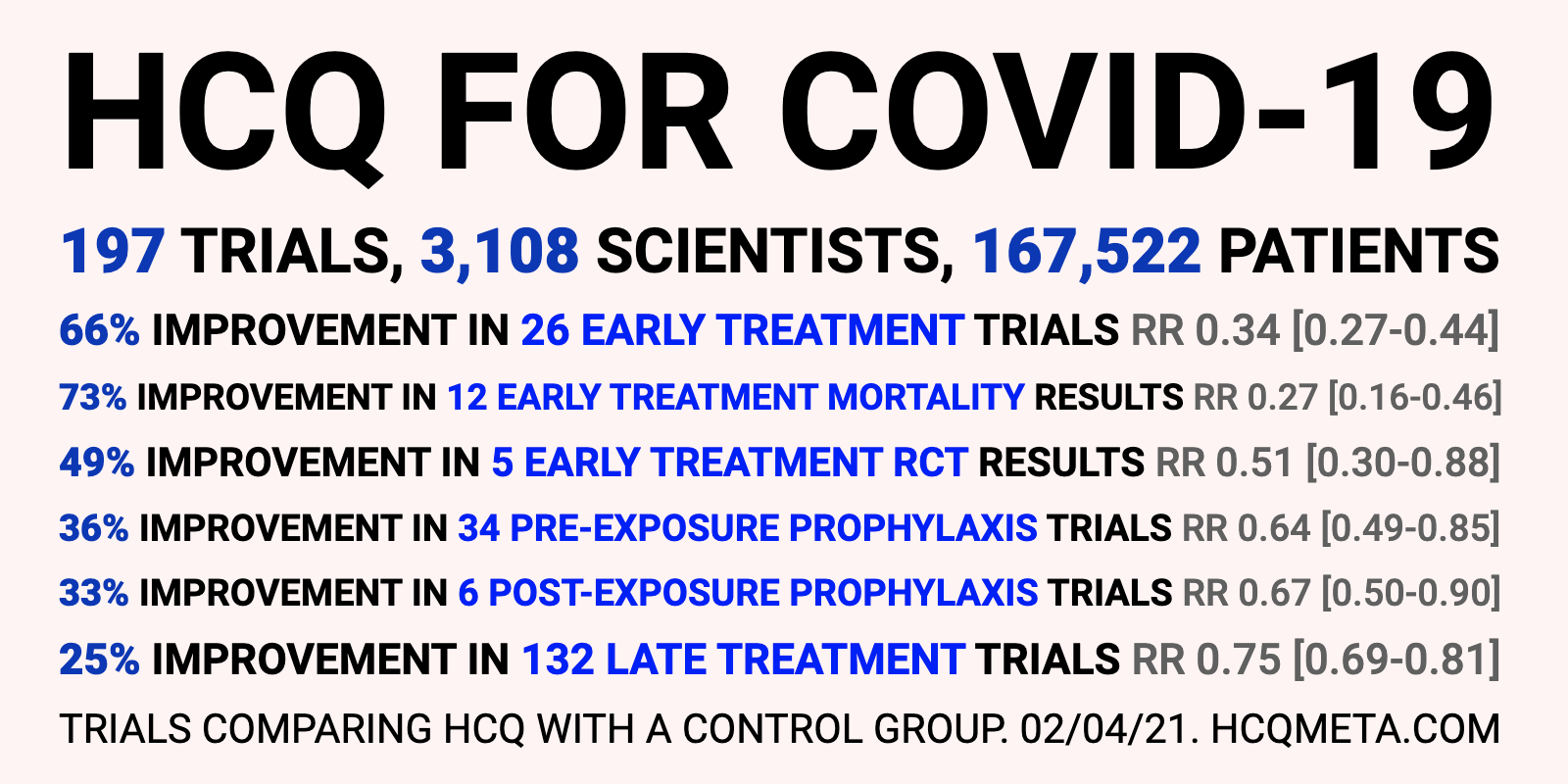 HCQ COVID-19 studies summary HCQ is effective for COVID-19 when used early: real-time meta analysis of 197 studiesCovid Analysis, Oct 20, 2020 (Version 64, Feb 2, 2021) https://hcqmeta.com/
IntroductionWe analyze all significant studies concerning the use of HCQ (or CQ) for COVID-19. Search methods, inclusion criteria, effect extraction criteria (more serious outcomes have priority), all individual study data, PRISMA answers, and statistical methods are detailed in Appendix 1. We present random-effects meta-analysis results for all studies, for studies within each treatment stage, for mortality results only, after exclusion of studies with critical bias, and for Randomized Controlled Trials (RCTs) only. Typical meta analyses involve subjective selection criteria and bias evaluation, requiring an understanding of the criteria and the accuracy of the evaluations. However, the volume of studies presents an opportunity for an additional simple and transparent analysis aimed at detecting efficacy. If treatment was not effective, the observed effects would be randomly distributed (or more likely to be negative if treatment is harmful). We can compute the probability that the observed percentage of positive results (or higher) could occur due to chance with an ineffective treatment (the probability of >= k heads in n coin tosses, or the one-sided sign test / binomial test). Analysis of publication bias is important and adjustments may be needed if there is a bias toward publishing positive results. For HCQ, we find evidence of a bias toward publishing negative results. Figure 2 shows stages of possible treatment for COVID-19. Pre-Exposure Prophylaxis (PrEP) refers to regularly taking medication before being infected, in order to prevent or minimize infection. In Post-Exposure Prophylaxis (PEP), medication is taken after exposure but before symptoms appear. Early Treatment refers to treatment immediately or soon after symptoms appear, while Late Treatment refers to more delayed treatment.  Figure 2. Treatment stages. Results Figure 3, Figure 4, and Table 1 show results by treatment stage, and Figure 5 shows a forest plot for a random effects meta-analysis of all studies. Early treatment. Late treatment. Pre-Exposure Prophylaxis. Post-Exposure Prophylaxis.
Table 1. Results by treatment stage. 3 studies report results for a subset with early treatment, these are not included in the overall results. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
Is Ivermectin The New Penicillin?by Tyler Durden 28May2021 – https://www.zerohedge.com/covid-19/ivermectin-new-penicillin Ivermectin, an anti-parasitic drug placed the same radioactive category as Hydroxychloroquine (HCQ) for the treatment of COVID-19, has reemerged as a promising treatment in the battle to extinguish the pandemic. New York Times best-selling author Michael Capuzzo has called it the “drug that cracked Covid,” writing that there are “hundreds of thousands, actually millions, of people around the world, from Uttar Pradesh in India to Peru to Brazil, who are living and not dying.” Doctors in India are big fans. To that end Dr. Justus R. Hope, MD asks in The Desert Review: Is Ivermectin the new Penicillin? As those Indian States using Ivermectin continue to diverge in cases and deaths from those states that forbid it, the natural experiment illustrates the power of Ivermectin decisively. Cases in Delhi, where Ivermectin was begun on April 20, dropped from 28,395 to just 2,260 on May 22. This represents an astounding 92% drop. Likewise, cases in Uttar Pradesh have dropped from 37,944 on April 24 to 5,964 on May 22 – a decline of 84%. Delhi and Uttar Pradesh followed the All India Institute of Medical Sciences (AIIMS) guidance published April 20, 2021, which called for dosing of .2 mg per kg of Ivermectin per body weight for three days. This amounts to 15 mg per day for a 150-pound person or 18 mg per day for a 200-pound individual. The other three Indian states that adopted it are all down as well. Goa is down from 4,195 to 1,647, Uttarakhand is down from 9,624 to 2,903, and Karnataka is down from 50,112 to 31,183. Goa adopted a pre-emptive policy of mass Ivermectin prevention for the entire adult population over age 18 at a dose of 12 mg daily for five days. Meanwhile, Tamil Nadu announced on May 14 they were outlawing Ivermectin in favor of the politically correct Remdesivir. As a result, Tamil Nadu’s cases are up in the same time frame from April 20 to May 22 – 10,986 to 35,873 – more than a tripling. Although Big Pharma and Big Media have scrambled to try, they cannot explain away this natural experiment. As I predicted May 12, they would first argue “the lockdowns worked.” The problem with this is that Tamil Nadu has been on strict lockdown for weeks as their cases have done nothing but climb. So the lockdown did not work. Their next argument was that “there has been a shift from the highly populated urban areas like Delhi and Mumbai” to the hinterlands, like Tamil Nadu. The big problem is that the adjacent state, Karnataka is just as rural, and its cases are dropping on Ivermectin. Uttar Pradesh is near the Himalayas and out in the far non-urbanized north where cases are down 84% with Ivermectin. Uttarakhand is even more rural and located in the Himalayas next to Nepal. Its infections are down 70% with Ivermectin. Their final argument lacked any proof. It was essentially an attempt to smear Ivermectin through association with another drug. It attempted to link Hydroxychloroquine (HCQ) with Ivermectin unfairly. While HCQ has become a punchline by the media, scientists like Dr. George Fareed know it is effective against COVID-19 – especially in the early stages. Dr. Fareed and his associate, Dr. Brian Tyson, have treated some 6,000 patients with nearly 100% success using a combination of HCQ, Ivermectin, Fluvoxamine, and various nutraceuticals, including zinc Vitamin D. Unfortunately, none of this has made it through the censorship of the mainstream media, and the public has not heard about the 200 plus studies that reflect HCQ’s effectiveness against COVID-19. The fact remains that HCQ has an undeserved negative connotation due to its connection with Trump, which is unfortunately used to tarnish other life-saving repurposed drugs, like Ivermectin. For example, in the recent Forbes article, journalist Ray uses the title, “Is Ivermectin the New Hydroxychloroquine?” Ray does not make a single substantive argument against Ivermectin; instead, he attempts to defame, debase or degrade it by repeating baseless accusations. For example, Ray cited Merck’s recommendation against Ivermectin as evidence of ineffectiveness, while Merck used no evidence to support their claim. In addition, he cited the FDA’s recommendation against Ivermectin, yet the FDA admits they have not reviewed the data on which to base this conclusion: “The FDA has not reviewed data to support the use of Ivermectin in COVID-19 patients to treat or prevent COVID-19…” As we all know, Merck was involved in the development of a competing drug and had 356 million reasons to throw its own cheap, unprofitable Ivermectin under the bus. Furthermore, the US government was likewise involved in a significant financial conflict of interest with Merck. The story of Ivermectin is more similar to that of Penicillin. Penicillin has saved almost 200 million lives. In addition, three men shared a Nobel Prize in 1945 for its discovery. Ivermectin’s discoverers won the 2015 Noble Prize in Medicine, and it has proven to be a life-saving drug in parasitic disease, especially in Africa. Over the past four decades, Ivermectin has saved millions from parasites like strongyloidiasis and onchocerciasis – river blindness. It has already saved tens of thousands from COVID-19 in India in those few locations that use it. It crashed Mexico’s, Slovakia’s, and Zimbabwe’s cases. I remain more convinced than ever that Ivermectin will bring an end to this Pandemic as the word gets out and more people share the book, Ivermectin for the World. A more fitting title to the Forbes piece might be, “Is Ivermectin the New Penicillin?” |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
By Justus R. Hope, MD 29June2021 https://www.thedesertreview.com/news/local/debating-ivermectin-hydroxychloroquine-and-colchicine/article_01fbb380-d917-11eb-91c2-73cdf82fa113.html  Colchicine is derived from the Autumn Crocus Plant Colchicine had been a Godsend drug to millions of gout sufferers worldwide – until the FDA stepped in and restricted its use. Colchicine, derived from the flowering autumn crocus plant, has been used since 1500 BC to treat joint swelling with exceptional pain-relieving properties. Like many natural gifts from God, like Ivermectin, this medication was regulated away from access to many in 2009 by the FDA. Before 2007, colchicine was widely, safely, and appropriately prescribed to some two million US patients each year at the cost of just 9 cents per pill. However, the FDA gained jurisdiction over all prescribed drugs in 1962 – ostensibly with the sole purpose of protecting the public. Some medications that were in widespread use before 1962, like colchicine, escaped this FDA approval. Therefore, in 2007, the FDA sought to remedy this problem by forcing a study to prove that colchicine truly worked and was safe to use. Never mind the real-world evidence accumulated by the practicing experts, the in-the-trenches physicians. So, Takeda Pharmaceuticals undertook this task, and tested the known drug colchicine in 184 patients, and guess what the study revealed? It answered the question that had already been answered. As expected, colchicine proved effective in gout, and it was effective in Familial Mediterranean Fever. In 2009, the FDA officially placed its rubber stamp of approval on the oral colchicine product, now known by the shiny new name of Colcrys. With the title came a price, and the cost of Colcrys was 5 dollars per pill – which was a 50 fold markup over the generic version. https://www.amazon.com/Surviving-Cancer-COVID-19-Disease-Repurposed/dp/0998055409 Suddenly most patients could no longer afford their colchicine. Many were forced to take less expensive, less effective, and more dangerous drugs instead. Dr. E. William Sinclair, president of the American College of Rheumatology (ACR), brought legal action against the FDA requesting that an affordable generic version be made available. After a legal battle, the court sided with the ACR. However, today the price of colchicine remains measured in terms of dollars, not cents. Other physician groups spoke in outrage. Dr. Aaron Kesselheim of Harvard Medical School was particularly vocal, “The way this case was handled has led to a potentially useful drug, colchicine, being prescribed to fewer patients, while there have been substantial cost increases for those who do use it and no evidence of a reduction in unsafe co-prescriptions.” Closely related to this are the now proposed “forced studies” by opponents of Ivermectin. WHO scientist and evidence-synthesis researcher Dr. Tess Lawrie’s peer-reviewed work is ranked in the top 5% of such scientists worldwide. She recently published the most comprehensive and authoritative meta-analysis on Ivermectin, analyzing some 24 randomized controlled trials involving 3406 patients. She concluded, “The findings indicate with moderate certainty that Ivermectin treatment in COVID-19 provides a significant survival benefit.” Dr. Lawrie commented about its overwhelming evidence of safety, “Ivermectin is not a new and experimental drug with an unknown safety profile. It is a WHO “Essential Medicine” already used in several different indications, in colossal cumulative volumes.” Safety concerns were disingenuously claimed by the WHO, the FDA, and even Merck. The WHO backed by the Gates Foundation, and Merck, who recently received 1.2 billion dollars for their new drug Molnupiravir (a competitor to Ivermectin), all expressed “safety concerns” with Ivermectin, and all three suffered massive financial conflicts of interest. Merck in particular, could not have been more aware of the contrary evidence from its own Mectizan Donation Program proving the drug to be exceedingly safe in billions of Mectizan doses since 1987. Dr. John Campbell called them out, “It is almost…as if they are saying that a drug (Ivermectin) known to be safe in one disease is somehow dangerous for another.” See the 16:50 mark. Dr. Campbell went on to explain that the basic science of Pharmacokinetics disproves this statement. He reiterated that if a drug has been deemed safe, as Ivermectin has, it cannot become unsafe.” Notwithstanding this, Dr. Lawrie stated the obvious in proposing its immediate use in the pandemic. “Given the evidence of efficacy, safety, low cost, and current death rates, Ivermectin is likely to have an impact on health and economic outcomes of the pandemic across many countries. Ivermectin is likely to be an equitable, acceptable, and feasible global intervention against COVID-19. Health professionals should strongly consider its use, in both treatment and prophylaxis.” Dr. Lawrie addressed the recent call for another study by Oxford, “By calling for more trials on Ivermectin in the current health emergency, our scientific advisers appear to have suspended their common sense. Let’s not suspend ours. Ivermectin is the key to restoring health and economies. We have nothing to lose by using safe old Ivermectin to save lives in this dire situation. The worst thing that can happen is that the global population is de-wormed. The best is that the health of people and nations is restored. Better safe than sorry.” Dr. Tess Lawrie has decades of experience in performing the technique of meta-analysis. The meta-analysis represents a pooling of multiple randomized controlled trials and deriving an overall signal. The meta-analysis ranks as the top form of medical evidence, and it even outranks the revered randomized controlled trial (RCT) that we have heard so much about. If the randomized controlled trial is the captain, then the meta-analysis is the admiral. Then why exactly is Oxford University touting their upcoming RCT when the world already has heard the answer from the meta-analysis performed by the best of the best, Dr. Tess Lawrie? Perhaps it is because Oxford, who famously backs the Astra Zeneca vaccine, has a financial conflict of interest. https://khn.org/news/rather-than-give-away-its-covid-vaccine-oxford-makes-a-deal-with-drugmaker/ If Ivermectin were approved, the Emergency Use Authorization for the experimental Astra Zeneca Vaccine would likely be voided. The Gates Foundation has taken a particular interest in “testing” Ivermectin. In addition to the Gates’ support of the Oxford Ivermectin Study, they are funding the TOGETHER Trial at none-other than McMaster University, the same one that botched the WHO Ivermectin review, and advised against the use of Ivermectin – all by using academic sleight of hand – by eliminating the favorable studies, and over-weighting the one neutral study. And by calling a precise result imprecise. Dr. Lawrie had this to say in her meta-analysis about the way the McMaster magicians made Ivermectin disappear, about the way they downgraded precision of a precise number by two levels without explanation, “The recently updated WHO therapeutics guidelines included seven trials and 1419 people in the analysis of mortality. Reporting a risk reduction of 81% (odds ratio 0.19, 95% CI 0.09–0.36), the effect estimate favoring Ivermectin was downgraded by two levels for imprecision, although the justification for this is unclear as the reported CI is precise (64%–91%).” The TIRC, the infamous Tobacco Industry Research Council, funded studies of tobacco that found results consistent with their interests. This resulted in more death and disease from cigarette smoking for five decades while the powerful tobacco lobby funded contrived studies. https://www.amazon.com/Emperor-All-Maladies-Biography-Cancer/dp/1439170916 We now see Oxford and McMaster trying hard to keep the EUA for vaccines alive amidst growing concerns of vaccine toxicity and variant escape. Will society stand by and allow Oxford and McMasters to subvert the overwhelming evidence already published in favor of Ivermectin? Dr. Tess Lawrie was clear in her IICC speech when she wisely stated, “Those who design the trials and control the data also control the outcome. So this system of industry-led trials needs to be put to an end. Data from ongoing and future trials of novel COVID treatments must be independently controlled and analyzed. Anything less than full transparency cannot be trusted.” See the 2:57 mark. Similarly, Yale’s Dr. Harvey Rich, Distinguished epidemiologist and Associate Editor of the Journal of the National Cancer Institute, has found alarming evidence of similar trials that were designed to fail in the case of Hydroxychloroquine (HCQ). In a presentation delivered on June 24, 2021, Dr. Risch discussed how the conflicts of interest drove tainted data and contrived-to-fail studies. He explained, “Randomized controlled trials are totally easy to subvert – in full public view. All you have to do is design them for unrealistic magnitudes of benefit, stop them early, use subjective outcomes or change outcomes in the middle of a trial or don’t validate the participants or their outcomes, ignore the medication shipping delays, use easily recognizable placebos so people can tell the difference, give inadequate or toxic doses, draw conclusions from part of the results and ignore inconvenient results, generalize the conclusions much wider than as applying to the actual subject, etc.” See the 18:25 mark. https://www.youtube.com/watch?v=x2DxP-6wHoY “Just to set the stage, I point out that Boulware had an active Pharma conflict of interest at the time he published these studies, but the author did not disclose those conflicts in the materials with the published papers. The conflicts were discovered from the documents found on the internet.” See the 24:10 mark. What Dr. Boulware failed to disclose in his 2020 HCQ publications was his research support from Gilead that he revealed in a 2019 conference, the ASTMH Annual Meeting on Tropical Medicine, given at National Harbor, Maryland. Dr. Risch went on to review nine studies from across the world associated with a 4-fold [75%] reduction in mortality [RR of .25 (0.19 – 0.34)] with HCQ used in early outpatient treatment in COVID-19. Dr. Risch summarized that the HCQ studies involved some 40,000 patients, and the magnitude of early outpatient treatment mortality reduction appeared even greater than with Ivermectin. See the 43:05 mark. https://www.youtube.com/watch?v=x2DxP-6wHoY These positive studies never made it to the mainstream media, unlike the subverted studies that demonized HCQ. The result of the deceptive studies was that the word of HCQ’s effectiveness never got out, and hundreds of thousands of lives were lost. Former Harvard Professor and NIH scientist Dr. George Fareed has treated outpatients with a cocktail including HCQ since the beginning of the pandemic and has received praise and appreciation from thousands whose lives he has saved. Most notably, Dr. Fareed and his dynamic young associate, Dr. Brian Tyson, would not be silenced, despite the adverse publicity on the drug. Their story, “The Miracle of the Imperial Valley,” has been published as a model for other physicians to follow: https://www.amazon.com/Ivermectin-World-Justus-R-Hope-ebook/dp/B0943T564G They have refined their cocktail with the addition of Ivermectin and Fluvoxamine, and various nutraceuticals. Dr. Fareed and Dr. Tyson together have now saved the lives of some 6,000 COVID-19 patients. There has been only one recorded death in a patient who presented late and did not receive the entire treatment course. There were only five hospitalizations. Let us acknowledge that Ivermectin reduces overall death by at least 62%, as Dr. Tess Lawrie has shown, and HCQ independently reduces it by 75%, as Dr. Risch has demonstrated. In that case, it is not surprising that the combination of the two drugs has reduced death by 99.98%, as the Fareed/Tyson series reveals. Some might question these numbers, thinking that the Ivermectin data should produce greater efficacy because of the numerous impressive natural experiments in India, Mexico, and Zimbabwe, showing 90+ percent reductions in cases and deaths. However, as Dr. Risch explains, we need to clarify precisely when these drugs are being used. We need to compare apples with apples. Dr. Risch confines his review to early outpatient treatment, while Dr. Lawrie looks at Ivermectin use across all phases, both inpatient and outpatient. Clearly, the reduction in death would be expected to be higher if the treatment review was confined to early in the outpatient phase rather than later in the hospital or the ICU. Ivermectin is proven to work well across all stages of the disease, including late in the cytokine storm, while HCQ works best early in the viral replication phase. Many case reports have shown that a single dose of Ivermectin can liberate a patient from the ventilator, even in the latest, worst stages of the disease. In India, the use of Ivermectin has been awe-inspiring. Within weeks of ICMR and AIIMS instituting Ivermectin on April 20, 2021, Delhi and Uttar Pradesh cases were down 99%. Goa famously chose Ivermectin in all adults over 18, and their cases are down 95% [4195 to 215]. Goa’s deaths peaked at 75 and are now 5, down 93%. See the JHU CSSE database. However, just as publicly, the Indian State of Tamil Nadu rejected Ivermectin and vowed to use Remdesivir instead. https://science.thewire.in/health/tn-revises-protocols-leaves-out-ivermectin-for-covid-patients/ They paid the price with the highest number of daily COVID-19 cases in India and excess deaths that continue to this day. As of June 26, 2021, there were 1258 deaths in India with a population of 1.36 billion. Tamil Nadu, with a population of 1/20 of India, saw 148 of these deaths, about 1/9 of India’s. This amounts to 80 excess deaths on June 26, 2021 [Predicted 1/20 of 1248 = 68. Actual = 148]. The question that emerges from Dr. Lawrie’s convincing meta-analysis and common sense when looking at Ivermectin’s massive benefit in those Indian States that used it is why any nation or state would want to repeat Tamil Nadu’s tragic error, and reject Ivermectin? Why would any area on earth wish to forego a treatment that works so well and is so safe? Uttar Pradesh, a state with 200 million inhabitants, an area that uses Ivermectin, by contrast, saw only 62 deaths. Uttar Pradesh, with 1/7 the population of India, did not experience 1/7 of the 1248 death toll, which would have been 178 lives [1/7 x 1248 = 178]. Instead, the Ivermectin saved at least 116 lives [Predicted deaths of 178 less actual deaths of 62 = 116 lives saved] just on June 26, 2021. Ivermectin reduces death in COVID-19 by a substantial percentage and with virtually no risk and minimal cost. Do we truly need more studies on Ivermectin while the Delta Variant rages on and vaccine resistance grows greater by the day? Do we need more studies on a drug that the world’s very best evidence – the meta-analysis – has proven reduces death by 62 to 91% and is safer than most vitamins? Why would we require a second-rate form of evidence, another RCT, when the gold-standard meta-analysis has already been published? We are asked to suspend our common sense while more people die and while Oxford and McMaster, both funded by the Gates Vaccine Foundation, make us wait on the result of another contrived-to-fail and forced study. Dr. Tess Lawrie has been aptly named “The Conscience of Medicine.” She has stood up against the WHO at great personal and professional cost to do what is right and moral and do what is in her patients’ best interests. She has chosen to honor her Hippocratic Oath. Like Dr. Roy Vagelos of Merck, Dr. Lawrie considers herself a physician first and foremost. Both individuals placed the interests of patients above those of money. Dr. Tess Lawrie closed her first annual International Ivermectin for COVID Conference with this passionate speech and these inspiring words to her fellow physicians, “And never before has our role as doctors been more important, because never before have we become complicit in potentially causing so much harm. I ask all doctors here today to look into their hearts and remember their (Hippocratic) Oath so that we can move forward, united in the protection of those we serve, and with the greatest of courage.” See the 7:33 mark. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
THIS NEEDS TO GO EVERYWHERE! 02September020 http://palmtreeofdeborah.blogspot.com/2020/09/this-needs-to-go-everywhere.html Analysis and presentation of the facts of the COVID-19 (SARS-CoV-2) Pandemic: Enough!Give backing to the Rabbonim who don’t want to go ahead with the decrees anymore.
[Excerpts from the letter] There is no place in Torah for a Jewish community to be governed by a committee of medical doctors. Nor by an unelected committee composed of Rabbonim, politicians and doctors. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
A President Betrayed by Bureaucrats: Scott Atlas Exposes The Real COVID Disasterby Tyler Durden 28November2021 – https://www.zerohedge.com/political/president-betrayed-bureaucrats-scott-atlas-exposes-real-covid-disaster Authored by Jeffrey Tucker via The Brownstone Institute, I’m a voracious reader of Covid books but nothing could have prepared me for Scott Atlas’s A Plague Upon Our House, a full and mind-blowing account of the famed scientist’s personal experience with the Covid era and a luridly detailed account of his time at the White House. The book is hot fire, from page one to the last, and will permanently affect your view of not only this pandemic and the policy response but also the workings of public health in general. 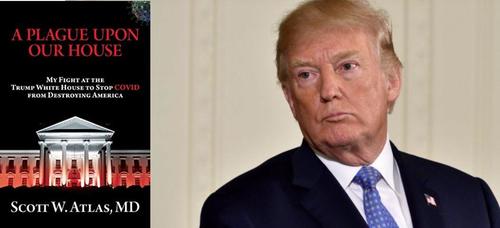 Scott Atlas’s A Plague Upon Our House Atlas’s book has exposed a scandal for the ages. It is enormously valuable because it fully blows up what seems to be an emerging fake story involving a supposedly Covid-denying president who did nothing vs. heroic scientists in the White House who urged compulsory mitigating measures consistent with prevailing scientific opinion. Not one word of that is true. Atlas’s book, I hope, makes it impossible to tell such tall tales without embarrassment. Anyone who tells you this fictional story (including Deborah Birx) deserves to have this highly credible treatise tossed in his direction. The book is about the war between real science (and genuine public health), with Atlas as the voice for reason both before and during his time in the White House, vs. the enactment of brutal policies that never stood any chance of controlling the virus while causing tremendous damage to the people, to human liberty, to children in particular, but also to billions of people around the world. For the reader, the author is our proxy, a reasonable and blunt man trapped in a world of lies, duplicity, backstabbing, opportunism, and fake science. He did his best but could not prevail against a powerful machine that cares nothing for facts, much less outcomes. If you have heretofore believed that science drives pandemic public policy, this book will shock you. Atlas’s recounting of the unbearably poor thinking on the part of government-based “infectious disease experts” will make your jaw drop (thinking, for example, of Birx’s off-the-cuff theorizing about the relationship between masking and controlling case spreads). Throughout the book, Atlas points to the enormous cost of the machinery of lockdowns, the preferred method of Anthony Fauci and Deborah Birx: missed cancer screenings, missed surgeries, nearly two years of educational losses, bankrupted small business, depression and drug overdoses, overall citizen demoralization, violations of religious freedom, all while public health massively neglected the actual at-risk population in long-term care facilities. Essentially, they were willing to dismantle everything we called civilization in the name of bludgeoning one pathogen without regard to the consequences. The fake science of population-wide “models” drove policy instead of following the known information about risk profiles.
“Restrictions on liberty were also destructive by inflaming class distinctions with their differential impact,” he writes, “exposing essential workers, sacrificing low-income families and kids, destroying single-parent homes, and eviscerating small businesses, while at the same time large companies were bailed out, elites worked from home with barely an interruption, and the ultra-rich got richer, leveraging their bully pulpit to demonize and cancel those who challenged their preferred policy options.” In the midst of continued chaos, in August 2020, Atlas was called by Trump to help, not as a political appointee, not as a PR man for Trump, not as a DC fixer but as the only person who in nearly a year of unfolding catastrophe had a health-policy focus. He made it clear from the outset that he would only say what he believed to be true; Trump agreed that this was precisely what he wanted and needed. Trump got an earful and gradually came around to a more rational view than that which caused him to wreck the American economy and society with his own hands and against his own instincts. In Task Force meetings, Atlas was the only person who showed up with studies and on-the-ground information as opposed to mere charts of infections easily downloadable from popular websites.
When Atlas spoke up, it was almost always to contradict Fauci/Birx but he received no backing during meetings, only to have many people in attendance later congratulate him for speaking out. Still, he did, by virtue of private meetings, have a convert in Trump himself, but by then it was too late: not even Trump could prevail against the wicked machine he had permissioned into operation. It’s a Mr. Smith Goes to Washington story but applied to matters of public health. From the outset of this disease panic, policy came to be dictated by two government bureaucrats (Fauci and Birx) who, for some reason, were confident in their control over media, bureaucracies, and White House messaging, despite every attempt by the president, Atlas, and a few others to get them to pay attention to the actual science about which Fauci/Birx knew and care little. When Atlas would raise doubts about Birx, Jared Kushner would repeatedly assure him that “she is 100% MAGA.” Yet we know for certain that this is not true. We know from a different book on the subject that she only took the position with the anticipation that Trump would lose the presidency in the November election. That’s hardly a surprise; it’s the bias expected from a career bureaucrat working for a deep-state institution. Fortunately, we now have this book to set the record straight. It gives every reader an inside look at the workings of a system that wrecked our lives. If the book finally declines to offer an explanation for the hell that was visited upon us – every day we still ask the question why? – it does provide an accounting of the who, when, where, and what. Tragically, too many scientists, media figures, and intellectuals in general went along. Atlas’s account shows exactly what they signed up to defend, and it’s not pretty. The cliche that kept coming to mind as I read is “breath of fresh air.” That metaphor describes the book perfectly: blessed relief from relentless propaganda. Imagine yourself trapped in an elevator with stultifying air in a building that is on fire and the smoke gradually seeps in from above. Someone is in there with you and he keeps assuring you that everything is fine, when it is obviously not. That’s a pretty good description of how I felt from March 12, 2020 and onward. That was the day that President Trump spoke to the nation and announced that there would be no more travel from Europe. The tone in his voice was spooky. It was obvious that more was coming. He had clearly fallen sway to extremely bad advice, perhaps he was willing to push lockdowns as a plan to deal with a respiratory virus that was already widespread in the US from perhaps 5 to 6 months earlier. It was the day that the darkness descended. A day later (March 13), the HHS distributed its lockdown plans for the nation. That weekend, Trump met for many hours with Anthony Fauci, Deborah Birx, son-in-law Jared Kushner, and only a few others. He came around to the idea of shutting down the American economy for two weeks. He presided over the calamitous March 16, 2020, press conference, at which Trump promised to beat the virus through general lockdowns. Of course he had no power to do that directly but he could urge it to happen, all under the completely delusional promise that doing so would solve the virus problem. Two weeks later, the same gang persuaded him to extend the lockdowns. Trump went along with the advice because it was the only advice he was fed at the time. They made it appear that the only choice that Trump had – if he wanted to beat the virus – was to wage war on his own policies that were pushing for a stronger, healthier economy. After surviving two impeachment attempts, and beating back years of hate from a nearly united media afflicted by severe derangement syndrome, Trump was finally hornswoggled. Atlas writes:
The truly tragic fact that both Republicans and Democrats do not want spoken about is that this whole calamity is that did indeed begin with Trump’s decision. On this point, Atlas writes:
Large parts of the narrative are devoted to explaining precisely how and to what extent Trump had been betrayed. “They had convinced him to do exactly the opposite of what he would naturally do in any other circumstance,” Atlas writes, that is
There are so many valuable parts to the story that I cannot possibly recount them all. The language is brilliant, e.g. he calls the media “the most despicable group of unprincipled liars one could ever imagine.” He proves that assertion in page after page of shocking lies and distortions, mostly driven by political goals. I was particularly struck by his chapter on testing, mainly because that whole racket mystified me throughout. From the outset, the CDC bungled the testing part of the pandemic story, attempting to keep the tests and process centralized in DC at the very time when the entire nation was in panic. Once that was finally fixed, months too late, mass and indiscriminate PCR testing became the desiderata of success within the White House. The problem was not just with the testing method:
The other problem is the wide assumption that more testing (however inaccurate) of whomever, whenever was always better. This model of maximizing tests seemed like a leftover from the HIV/AIDS crisis in which tracing was mostly useless in practice but at least made some sense in theory. For a widespread and mostly wild respiratory disease transmitted the way a cold virus is transmitted, this method was hopeless from the beginning. It became nothing but make work for tracing bureaucrats and testing enterprises that in the end only provided a fake metric of “success” that served to spread public panic. Early on, Fauci had clearly said that there was no reason to get tested if you had no symptoms. Later, that common-sense outlook was thrown out the window and replaced with an agenda to test as many people as possible regardless of risk and regardless of symptoms. The resulting data enabled Fauci/Birx to keep everyone in a constant state of alarm. More test positivity to them implied only one thing: more lockdowns. Businesses needed to close harder, we all needed to mask harder, schools needed to stay closed longer, and travel needed to be ever more restricted. That assumption became so entrenched that not even the president’s own wishes (which had changed from Spring to Summer) made any difference. Atlas’s first job, then, was to challenge this whole indiscriminate testing agenda. To his mind, testing needed to be about more than accumulating endless amounts of data, much of it without meaning; instead, testing should be directed toward a public-health goal. The people who needed tests were the vulnerable populations, particularly those in nursing homes, with the goal of saving lives among those who were actually threatened with severe outcomes. This push to test, contact trace, and quarantine anyone and everyone regardless of known risk was a huge distraction, and also caused huge disruption in schooling and enterprise. To fix it meant changing the CDC guidelines. Atlas’s story of attempting to do that is eye-opening. He wrestled with every manner of bureaucrat and managed to get new guidelines written, only to find that they had been mysteriously reverted to the old guidelines one week later. He caught the “error” and insisted that his version prevail. Once they were issued by the CDC, the national press was all over it, with the story that the White House was pressuring the scientists at the CDC in terrible ways. After a week-long media storm, the guidelines changed yet again. All of Atlas’s work was made null. Talk about discouraging! It was also Atlas’s first full experience in dealing with deep-state machinations. It was this way throughout the lockdown period, a machinery in place to implement, encourage, and enforce endless restrictions but no one person in particular was there to take responsibility for the policies or the outcomes, even as the ostensible head of state (Trump) was on record both publicly and privately opposing the policies that no one could seem to stop. As an example of this, Atlas tells the story of bringing some massively important scientists to the White House to speak with Trump: Martin Kulldorff, Jay Bhattacharya, Joseph Ladapo, and Cody Meissner. People around the president thought the idea was great. But somehow the meeting kept being delayed. Again and again. When it finally went ahead, the schedulers only allowed for 5 minutes. But once they met with Trump himself, the president had other ideas and prolonged the meeting for an hour and a half, asking the scientists all kinds of questions about viruses, policy, the initial lockdowns, the risks to individuals, and so on. The president was so impressed with their views and knowledge – what a dramatic change that must have been for him – that he invited filming to be done plus pictures to be taken. He wanted to make it a big public splash. It never happened. Literally. White House press somehow got the message that this meeting never happened. The first anyone will have known about it other than White House employees is from Atlas’s book. Two months later, Atlas was instrumental in bringing in not only two of those scientists but also the famed Sunetra Gupta of Oxford. They met with the HHS secretary but this meeting too was buried in the press. No dissent was allowed. The bureaucrats were in charge, regardless of the wishes of the president. Another case in point was during Trump’s own bout with Covid in early October. Atlas was nearly sure that he would be fine but he was forbidden from talking to the press. The entire White House communications office was frozen for four days, with no one speaking to the press. This was against Trump’s own wishes. This left the media to speculate that he was on his deathbed, so when he came back to the White House and announced that Covid is not to be feared, it was a shock to the nation. From my own point of view, this was truly Trump’s finest moment. To learn of the internal machinations happening behind the scenes is pretty shocking. I can’t possibly cover the wealth of material in this book, and I expect this brief review to be one of several that I write. I do have a few disagreements. First, I think the author is too uncritical toward Operation Warp Speed and doesn’t really address how the vaccines were wildly oversold, to say nothing of growing concerns about safety, which were not addressed in the trials. Second, he seems to approve of Trump’s March 12th travel restrictions, which struck me as brutal and pointless, and the real beginning of the unfolding disaster. Third, Atlas inadvertently seems to perpetuate the distortion that Trump recommended ingesting bleach during a press conference. I know that this was all over the papers. But I’ve read the transcript of that press conference several times and find nothing like this. Trump actually makes clear that he was speaking about cleaning surfaces. This might be yet another case of outright media lies. All that aside, this book reveals everything about the insanity of 2020 and 2021, years in which good sense, good science, historical precedent, human rights, and concerns for human liberty were all thrown into the trash, not just in the US but all over the world. Atlas summarizes the big picture:
Atlas is correct that “the management of this pandemic has left a stain on many of America’s once noble institutions, including our elite universities, research institutes and journals, and public health agencies. Earning it back will not be easy.” Internationally, we have Sweden as an example of a country that (mostly) kept its sanity. Domestically, we have South Dakota as an example of a place that stayed open, preserving freedom throughout. And thanks in large part to Atlas’s behind-the-scenes work, we have the example of Florida, whose governor did care about the actual science and ended up preserving freedom in the state even as the elderly population there experienced the greatest possible protection from the virus. We all owe Atlas an enormous debt of gratitude, for it was he who persuaded the Florida governor to choose the path of focussed protection as advocated by the Great Barrington Declaration, which Atlas cites as the “single document that will go down as one of the most important publications in the pandemic, as it lent undeniable credibility to focused protection and provided courage to thousands of additional medical scientists and public health leaders to come forward.” Atlas experienced the slings, arrows, and worse. The media and the bureaucrats tried to shut him up, shut him down, and body bag him professionally and personally. Cancelled, meaning removed from the roster of functional, dignified human beings. Even colleagues at Stanford University joined in the lynch mob, much to their disgrace. And yet this book is that of a man who has prevailed against them. In that sense, this book is easily the most crucial first-person account we have so far. It is gripping, revealing, devastating for the lockdowners and their vaccine-mandating successors, and a true classic that will stand the test of time. It’s simply not possible to write the history of this disaster without a close examination of this erudite first-hand account. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
COVID-19 TESTING: The Lies they Tell
Why Hardly Anyone Trusts The Virus ‘Experts’by Tyler Durden Tuesday, Jan 19, 2021 – 10:05 https://www.zerohedge.com/covid-19/why-hardly-anyone-trusts-virus-experts Authored by John Rubino via DollarCollapse.com, Early in the pandemic, “trust the science!” could actually be used in a debate without attracting derisive laughter. But as the flip-flops, mistakes and, yes, lies have accumulated, a consensus seems to be forming that the health care authorities are no more trustworthy than the people running Congress or the Fed. For proof, let’s start with vitamin D, which sure seems to lessen the severity of coronavirus infections. As the chart below illustrates (couldn’t find the source, but google “covid vitamin D” and you’ll find lots of studies that track with this data), people with higher levels of vitamin D in their bloodstream tend to experience covid-19 as a non-event while people low levels found the infection life-threatening.
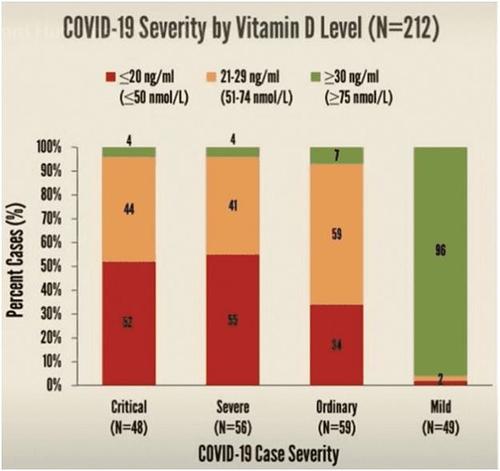 Vitamin D and covid 2021
There are obvious questions about causality here, so calling vitamin D a “cure” is going way too far. But if it has even a marginal effect – and the data suggest considerably more — a rational government would, you’d think, be handing out vitamin D like Halloween candy. In fact, since we’re mandating/prohibiting all kinds of other behaviors, we might expect vitamin D consumption to be required along with masks and social distancing. Even covid-czar Anthony Fauci recently said:
So why aren’t family-sized bottles of vitamin D arriving in the mail from the CDC? A cynic might wonder if the fact that Big Pharma doesn’t make much money from cheap, widely available supplements plays a role in the government’s apparent lack of interest. Now about those lockdowns. Tom Woods has been producing charts that appear to show virtually no difference in virus outcomes between US states with aggressive lockdown policies and those without. California, for instance, has shuttered most of its small businesses and imposed widespread curfews, while Florida hasn’t. Here’s the result:
 California vs Florida covid lockdowns
As for the rest of the world – where they’re supposedly doing better than the US – the pattern of zero correlation between lockdowns and virus spread seems to be holding. France imposed a full national lockdown in March – after which the virus spiked. Then they added mask mandates (indoor and outdoor), with fines attached. And daily new cases soared.
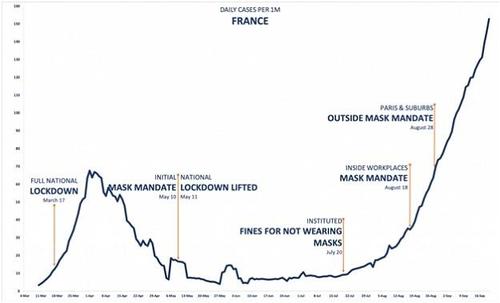 France covid 2021
Then of course there’s the lying. Dr. Fauci first claimed that masks don’t help – when he believed they did help — because he feared mask shortages for health care workers. He also admits to changing the official line on herd immunity according to what he thinks we’re ready to hear. And, in what sounds more like incompetence than dishonesty, he’s apparently been answering the question “when will life go back to normal?” with whatever pops into his head at the time. In early 2020, it was the coming Autumn. In July, it was “a year or so.” More recently it’s “well into 2021.” But the biggest and by far the most outrageous reason for this growing mistrust has to be the World Health Organization which, well, read for yourself:
The health care establishment could have saved a lot of time — and embarrassment — by just asking regular people about this stuff. But then they would have made a lot less money. |
|
|
|
Casedemic: The Hideous Scandal Of The Irredeemably Flawed PCR Testby Tyler Durden 06December2021 – https://www.zerohedge.com/covid-19/casedemic-hideous-scandal-irredeemably-flawed-pcr-test Authored by Ian McNulty via The Brownstone Institute, Investigating the cause of a disease is like investigating the cause of a crime. Just as the detection of a suspect’s DNA at a crime scene doesn’t prove they committed the crime, so the detection of the DNA of a virus in a patient doesn’t prove it caused the disease. Consider the case of Epstein-Barr Virus (EBV) for example. It can cause serious diseases like arthritis, multiple sclerosis and cancer. A Japanese study in 2003 found that 43% of patients suffering from Chronic Active Epstein-Barr Virus (CAEBV) died within 5 months to 12 years of infection. Yet EBV is one of the most common viruses in humans and has been detected in 95% of the adult population. Most of those infected are either asymptomatic or show symptoms of glandular fever, which can have similar symptoms to ‘long Covid.’ If an advertising agency attempted to create demand for an EBV treatment with daily TV and radio ads representing positive EBV tests as ‘EBV Cases’ and deaths within 28 days as ‘EBV Deaths,’ they’d be prosecuted for fraud by false representation so quickly their feet wouldn’t touch the ground.
 No-Yes blocks
How Viruses Are DetectedBefore the invention of PCR, the gold standard for detecting viruses was to grow them in a culture of living cells and count damaged cells using a microscope. The disadvantage of cell cultures is they need highly skilled technicians and can take weeks to complete. The advantage is they only count living viruses that multiply and damage cells. Dead virus fragments that do neither are automatically discounted. The invention of PCR in 1983 was a game changer. Instead of waiting for viruses to grow naturally, PCR rapidly multiplies tiny amounts of viral DNA exponentially in a series of heating and cooling cycles that can be automated and completed in less than an hour. PCR revolutionised molecular biology but its most notable application was in genetic fingerprinting, where its ability to magnify even the smallest traces of DNA became a major weapon in the fight against crime. But, like a powerful magnifying glass or zoom lens, if it’s powerful enough to find a needle in a haystack it’s powerful enough to make mountains out of molehills. Even the inventor of PCR, Kary Mullis, who won the Nobel Prize in Chemistry in 1993, vehemently opposed using PCR to diagnose diseases: “PCR is a process that’s used to make a whole lot of something out of something. It allows you to take a very miniscule amount of anything and make it measurable and then talk about it like it’s important.“ PCR has certainly allowed public health authorities and the media around the world to talk about a new variant of Coronavirus like it’s important, but how important is it really? The Dose Makes The PoisonAnything can be deadly in high enough doses, even oxygen and water. Since the time of Paracelsus in the 16th century, science has known there are no such things as poisons, only poisonous concentrations:
This basic principle is expressed in the adage “dosis sola facit venenum“ – the dose alone makes the poison – and is the basis for all Public Health Standards which specify Maximum Permissible Doses (MPDs) for all known health hazards, from chemicals and radiation to bacteria, viruses and even noise. Public Health Standards, Science and LawToxicology and Law are both highly specialised subjects with their own highly specialised language. Depending on the jurisdiction, Maximum Permissible Doses (MPDs) are also known as Health Based Exposure Limits (HBELs), Maximum Exposure Levels (MELs) and Permissible Exposure Limits (PELs). But, no matter how complicated and confusing the language, the basic principles are simple. If the dose alone makes the poison then it’s the dose that’s the biggest concern, not the poison. And if Public Health Standards in a liberal democracy are regulated by the rule of law then the law needs to be simple enough for a jury of reasonably intelligent lay people to understand. Although the harm caused by any toxin increases with the dose, the level of harm depends not only on the toxin, but the susceptibility of the individual and the way the toxin is delivered. Maximum Permissible Doses have to strike a balance between the benefit of increasing safety and the cost of doing it. There are many Political, Economic and Social factors to consider besides the Technology (PEST). Take the case of noise for example. The smallest whisper may be irritating and harmful to some people, while the loudest music may be nourishing and healthy for others. If the Maximum Permissible Dose was set at a level to protect the most sensitive from any risk of harm, life would be impossible for everyone else. Maximum Permissible Doses have to balance the costs and benefits of restricting exposure to the level of No Observable Effect (NOEL) at one end of the scale, and the level that would kill 50% of the population at the other (LD50). Bacteria and viruses are different from other toxins, but the principle is the same. Because they multiply and increase their dose with time, maximum permissible doses need to be based on the minimum dose likely to start an infection known as the Minimum Infective Dose (MID). Take the case of listeria monocytogenes for example. It’s the bacteria that causes listeriosis, a serious disease that can result in meningitis, sepsis and encephalitis. The case fatality rate is around 20%, making it ten times more deadly than Covid-19. Yet listeria is widespread in the environment and can be detected in raw meat and vegetables as well as many ready-to-eat foods, including cooked meat and seafood, dairy products, pre-prepared sandwiches and salads. The minimum dose in food likely to cause an outbreak of listeriosis is around 1,000 live bacteria per gram. Allowing a suitable margin of safety, EU and US food standards set the maximum permissible dose of listeria in ready-to-eat products at 10% of the minimum infective dose , or 100 live bacteria per gram. If Maximum Permissible Doses were based solely on the detection of a bacteria or virus rather than the dose, the food industry would cease to exist. Protection of the VulnerableThe general rule of thumb for setting maximum permissible doses used to be 10% of the MID for bacteria and viruses, and 10% of the LD50 for other toxins, but this has come under increasing criticism in recent years: first with radiation, then Environmental Tobacco Smoke (ETS), then smoke in general, then viruses. The idea that there is no safe dose of some toxins began to surface in the 1950s, when radioactive fallout from atom bomb tests and radiation from medical X-rays were linked with the the dramatic post-war rise in cancers and birth defects. Although this was rejected by the science at the time, it wasn’t entirely unfounded. There are many reasons why radiation may be different from other pollutants. Chemicals like carbon, oxygen, hydrogen and nitrogen are recycled naturally by the environment, but there is no such thing as a Radiation Cycle. Radioactivity only disappears gradually with time, no matter how many times it’s recycled. Some radioactive substances remain dangerous for periods longer than human history. All life forms are powered by chemical processes, none by nuclear energy. The last natural nuclear reactor on earth burned out more than 1.5 billion years ago. The nearest one now is isolated from life on earth by 93 million miles of vacuum. As evidence mounted to show there was no safe dose of radiation, maximum permissible doses were lowered drastically, but limited doses were still allowed. If public health standards were based purely on the detection of radiation rather than the dose, the Nuclear Industry would cease to exist. The susceptibility of any individual to any health risk depends on many factors. Most people can eat sesame seeds and survive bee stings without calling an ambulance, for others they can be fatal. In the US bees and wasps kill an average of more than 60 people each year, and food allergies cause an average of 30,000 hospitalisations and 150 deaths. If public health standards were based solely on the detection of a toxin rather than the dose, all bees would be exterminated and all food production closed down. Food allergies set the legal precedent. Where minuscule traces of something might be harmful for some people, the law demands that products carry a clear warning to allow the vulnerable to protect their own health. It doesn’t demand everyone else pay the price, no matter what the cost, by lowering maximum permissible doses to the point of no observable effect. Minimum Infectious Doses (MIDs) have already been established for many of the major respiratory and enteric viruses including strains of coronavirus. Even though SARS-CoV-2 is a new variant of coronavirus, the MID has already been estimated at around 100 particles. Whilst further work is needed, nevertheless it could serve as a working standard to measure Covid-19 infections against. Are PCR Numbers Scientific?As the philosopher of science, Karl Popper, observed: “non-reproducible single occurrences are of no significance to science.” To be reproducible, the results of one test should compare within a small margin of error with the results of other tests. To make this possible all measuring instruments are calibrated against international standards. If they aren’t, their measurements may appear to be significant, but they have no significance in science. PCR tests magnify the number of target DNA particles in a swab exponentially until they become visible. Like a powerful zoom lens, the greater the magnification needed to see something, the smaller it actually is. The magnification in PCR is measured by the number of cycles needed to make the DNA visible. Known as the Cycle Threshold (Ct) or Quantification Cycle (Cq) number, the higher the number of cycles the lower the amount of DNA in the sample. To convert Cq numbers into doses they have to be calibrated against the Cq numbers of standard doses. If they aren’t they can easily be blown out of proportion and appear more significant than they actually are. Take an advertisement for a car for example. With the right light, the right angle and the right magnification, a scale model can look like the real thing. We can only gauge the true size of things if we have something to measure them against. Just like a coin standing next to a toy car proves it’s not a real one, and a shoe next to a molehill shows it’s not a mountain, the Cq of a standard dose next to the Cq of a sample shows how big the dose really is. So it’s alarming to discover that there are no international standards for PCR tests and even more alarming to discover that results can vary up to a million fold, not just from country to country, but from test to test. Even though this is well-documented in the scientific literature it appears that the media, public health authorities and government regulators either haven’t noticed or don’t care:
Even the CDC itself admits PCR test results aren’t reproducible:
For this reason PCR tests are licenced under emergency regulations for the detection of the type or ‘quality’ of a virus, not for the dose or ‘quantity’ of it.
Just because we can detect the ‘genetic fingerprint’ of a virus doesn’t prove it’s the cause of a disease:
So, while there’s little doubt that using PCR to identify the genetic fingerprint of a Covid-19 virus is the gold standard in molecular science, there’s equally no doubt that using it as the gold standard to quantify Covid-19 ‘cases’ and ‘deaths’ is “ill-advised.” The idea that PCR may have been used to make a mountain out of a molehill by blowing a relatively ordinary disease outbreak out of all proportion is so shocking it’s literally unthinkable. But it wouldn’t be the first time it has happened. The Epidemic That Wasn’tIn spring 2006 staff at the Dartmouth-Hitchcock Medical Center in New Hampshire began showing symptoms of respiratory infection with high fever and nonstop coughing that left them gasping for breath and lasted for weeks. Using the latest PCR techniques, Dartmouth-Hitchcock’s laboratories found 142 cases of pertussis or whooping cough, which causes pneumonia in vulnerable adults and can be deadly for infants. Medical procedures were cancelled, hospital beds were taken out of commission. Nearly 1,000 health care workers were furloughed, 1,445 were treated with antibiotics and 4,524 were vaccinated against whooping cough. Eight months later, when the state health department had completed the standard culture tests, not one single case of whooping cough could be confirmed. It seems Dartmouth-Hitchcock had suffered an outbreak of ordinary respiratory diseases no more serious than the common cold! The following January the New York Times ran the story under the headline “Faith in Quick Test Leads to Epidemic That Wasn’t.” “Pseudo-epidemics happen all the time,” said Dr. Trish Perl, past president of the Society of Epidemiologists of America. “It’s a problem; we know it’s a problem. My guess is that what happened at Dartmouth is going to become more common.” “PCR tests are quick and extremely sensitive, but their very sensitivity makes false positives likely” reported the New York Times, “and when hundreds or thousands of people are tested, as occurred at Dartmouth, false positives can make it seem like there is an epidemic.” “To say the episode was disruptive was an understatement,” said Dr. Elizabeth Talbot, deputy epidemiologist for the New Hampshire Department of Health, “I had a feeling at the time that this gave us a shadow of a hint of what it might be like during a pandemic flu epidemic.” Dr. Cathy A. Petti, an infectious disease specialist at the University of Utah, said the story had one clear lesson. “The big message is that every lab is vulnerable to having false positives. No single test result is absolute and that is even more important with a test result based on PCR.” The Swine Flu Panic of 2009In the spring of 2009 a 5-year old boy living near an intensive pig farm in Mexico went down with an unknown disease that caused a high fever, sore throat and whole body ache. Several weeks later a lab in Canada tested a nasal swab from the boy and discovered a variant of the flu virus similar to the H1N1 Avian flu virus which they labelled H1N1/09, soon to be known as ‘Swine Flu.’ On 28 April 2009 a biotech company in Colorado announced they had developed the MChip, a version of the FluChip, which enabled PCR tests to distinguish the Swine Flu H1N1/09 virus from other flu types. “Since the FluChip assay can be conducted within a single day,” said InDevR’s leading developer and CEO, Prof Kathy Rowlen, “it could be employed in State Public Health Laboratories to greatly enhance influenza surveillance and our ability to track the virus.” Up until this point the top of the World Health Organisation (WHO) Pandemic Preparedness homepage had carried the statement:
Less than a week after the MChip announcement, the WHO removed the phrase “enormous numbers of deaths and illness,” to require only that “a new influenza virus appears against which the human population has no immunity” before a flu outbreak to be called a ‘pandemic.’ No sooner had the laboratories started PCR testing with MChip than they were finding H1N1/09 everywhere. By the beginning of June almost three-quarters of all influenza cases tested positive for Swine Flu. Mainstream news reported the rise in cases on a daily basis, comparing it with the H1N1 Avian Flu pandemic in 1918 which killed more than 50 million people. What they neglected to mention is that, although they have similar names, Avian Flu H1N1 is very different and much more deadly than Swine Flu H1N1/09 . Even though there had been less than 500 deaths up to this point compared to more than 20,000 deaths in a severe flu epidemic people flocked to health centres demanding to be tested, producing even more positive ‘cases,’ In mid-May senior representatives of all the major pharmaceutical companies met with WHO Director-General, Margaret Chan, and UN Secretary General, Ban Ki Moon, to discuss delivery of swine flu vaccines. Many contracts had already been signed. Germany had a contract with GlaxoSmithKline (GSK) to buy 50 million doses at a cost of half a billion Euros which came into effect automatically the moment a pandemic was declared. The UK bought 132 million doses – two for every person in the country. On 11 June 2009 WHO Director-General Margaret Chan, announced:
On 16 July the Guardian reported that swine flu was spreading fast across much of the UK with 55,000 new cases the previous week in England alone. The UK’s Chief Medical Officer, Professor Sir Liam Donaldson, warned that in the worst case scenario 30% of the population could be infected and 65,000 killed. On 20 July a study in The Lancet co-authored by WHO and UK government adviser, Neil Ferguson, recommended closing schools and churches to slow the epidemic, limit stress on the NHS and “give more time for vaccine production.” On the same day WHO Director-General, Margaret Chan announced that “vaccine makers could produce 4.9 billion pandemic flu shots per year in the best-case scenario.” Four days later an official Obama administration spokesman warned that “as many as several hundred thousand could die if a vaccine campaign and other measures aren’t successful.” The warnings had the desired effect. That week UK consultation rates for influenza-like illnesses (ILIs) were at their highest since the last severe flu epidemic in 1999/2000, even though death rates were at a 15-year low. On 29 September 2009 the Pandemrix vaccine from GlaxoSmithKline (GSK) was rushed through European Medicines Agency approval, swiftly followed by Baxter’s Celvapan the following week. On 19 November the WHO announced that 65 million doses of vaccine had been administered worldwide. As the year drew to a close it became increasingly obvious that swine flu was not all it was made out to be. The previous winter (2008/2009) the Office for National Statistics (ONS) had reported 36,700 excess deaths in England and Wales, the highest since the last severe flu outbreak of 1999/2000. Even though the winter of 2009 had been the coldest for 30 years, excess deaths were 30% lower than the previous winter. Whatever swine flu was, it wasn’t as deadly as other flu variants. On 26 January the following year, Wolfgang Wodarg, a German doctor and member of parliament, told the European Council in Strasbourg that the major global pharmaceutical corporations had organised a “campaign of panic” to sell vaccines, putting pressure on the WHO to declare what he called a “false pandemic” in “one of the greatest medicine scandals of the century.” “Millions of people worldwide were vaccinated for no good reason,” said Wodarg, boosting pharmaceutical company profits by more than $18 billion. Annual sales of Tamiflu alone had jumped 435 percent, to €2.2 billion. By April 2010, it was apparent that most of the vaccines were not needed. The US government had bought 229 million doses of which only 91 million doses were used. Of the surplus, some of it was stored in bulk, some of it was sent to developing countries and 71 million doses were destroyed. On 12 March 2010 SPIEGEL International published what it called “Reconstruction of a Mass Hysteria” that ended with a question:
But it didn’t take long to find an answer. In December the Independent published a story with the headline “Swine flu, the killer virus that actually saved lives.”
Instead of the low death rate proving that swine flu had been a fake pandemic, confidence in the organisations that had “gambled away precious confidence” was quickly restored by portraying swine flu as something that “actually saved lives” by driving out the common flu. PCR and LawPortraying something as something it isn’t is deception. Doing it for profit is fraud. Doing it by first gaining the trust of the victims is a confidence trick or a con. In England, Wales and Northern Ireland fraud is covered by the Fraud Act 2006 and is divided into three classes – ‘fraud by false representation,’ ‘fraud by failing to disclose information’ and ‘fraud by abuse of position.’ A representation is false if the person making it knows it may be untrue or misleading. If they do it for amusement, it’s a trick or a hoax. If they do it to make a gain, or expose others to a risk of loss, it’s ‘fraud by false representation.’ If someone has a duty to disclose information and they don’t do it, it might be negligence or simple incompetence. If they do it to make a gain, or expose others to a risk of loss, it’s ‘fraud by failing to disclose information.’ If they occupy a position where they are expected not to act against the interests of others, and do it to make a gain or expose others to a risk of loss, it’s ‘fraud by abuse of position.’ In Dartmouth Hitchcock’s case there’s no doubt that using PCR to identify a common respiratory infection as whooping cough was ‘false representation,’ but it was an honest mistake, made with the best of intentions. If any gain was intended it was to protect others from risk of loss, not to expose them to it. There was no failure to disclose information and nobody abused their position. In the case of swine flu things aren’t so clear. By 2009 there were already plenty of warnings from Dartmouth Hitchcock and many other similar incidents that using PCR to detect the genetic fingerprint of a bacteria or virus may be misleading. Worse still, the potential of PCR to magnify things out of all proportion creates opportunities for all those who would gain by making mountains out of molehills and global pandemics out of relatively ordinary seasonal epidemics. The average journalist, lawyer, member of parliament or member of the public may be forgiven for not knowing about the dangers of PCR, but public health experts had no excuse. It may be argued that their job is to protect the public by erring on the side of caution. It may equally be argued that the massive amounts of money spent by global pharmaceutical corporations on marketing, public relations and lobbying creates enormous conflicts of interest, increasing the potential for suppression of information and abuse of position across all professions, from politics and journalism to education and public health. The defence is full disclosure of all information, particularly on the potential of PCR to identify the wrong culprit in an infection and blow it out of all proportion. The fact this was never done is suspicious. If there were any prosecutions for fraud they weren’t widely publicised, and if there were any questions raised or lessons to be learned about the role of PCR in creating the 2009 Swine Flu panic they were quickly forgotten. The First Rough Draft of HistoryThe first rough attempt to represent things in the outside world is journalism. But no representation can be 100% true. ‘Representation’ is literally a re-presentation of something that symbolises or ‘stands in for’ something else. Nothing can fully capture every aspect of a thing except the thing itself. So judging whether a representation is true or false depends on your point of view. It’s a matter of opinion, open to debate in other words. In a free and functioning democracy the first line of defence against false representation is a free and independent press. Where one news organisation may represent something as one thing, a competing organisation may represent it as something completely different. Competing representations are tried in the court of public opinion and evolve by a process of survival of the fittest. Whilst this may be true in theory, in practice it isn’t. Advertising proves people choose the most attractive representations, not the truest. News organisations are funded by financiers who put their own interests first, not the public’s. Whether the intention is to deliberately defraud the public or simply to sell newspapers by creating controversy, the potential for false representations is enormous. Trial By MediaDespite the CDC’s own admission that PCR tests “may not indicate the presence of infectious virus,” its use to do exactly that in the case of Covid was accepted without question. Worse still, the measures taken against calling PCR into question have become progressively more draconian and underhanded since the very beginning. The mould was set with the announcement of the first UK death on Saturday 29 February 2020. Every newspaper in Britain carried the same front page story: “EMERGENCY laws to tackle coronavirus are being rushed in after the outbreak claimed its first British life yesterday,” screamed The Daily Mail.
 EMERGENCY laws to tackle coronavirus are being rushed in after the outbreak claimed its first British life yesterday
The first British victim contracted the virus on the Diamond Princess cruise ship in Japan, not Britain, but it didn’t matter. With less than 20 cases in the UK and one ‘British’ death in Japan, the media had already decided it justified rushing in emergency laws. How did they know how dangerous it was? How were they able to predict the future? Had they forgotten the lessons of the 2009 Swine Flu panic? After almost 2 weeks of newspaper, TV and radio fearmongering, Prime Minister Boris Johnson made it official at the Downing Street press conference on Thursday 12 March 2020 when he said:
None of that statement stood up to scrutiny, but none of the hand-picked journalists in the room had the right knowledge to ask the right questions. After 20 minutes blinding the press and public with science, Johnson opened the floor to questions. The first question, from the BBC’s Laura Kuenssberg, set the mould by accepting the Prime Minister’s statement without question:
Any journalist who remembered the 2009 Swine Flu panic, might have asked how the PM knew, after just 10 deaths, that it was the worst public health crisis in a generation? He didn’t say it may be or could be but definitely ‘is.’ Did he have a crystal ball? Or was he following the same Imperial College modelling that had predicted 136,000 deaths from mad cow disease in 2002, 200 million deaths from bird flu in 2005 and 65,000 deaths from swine flu in 2009, all of which had proved completely wrong? As the BBC’s chief political correspondent Kuenssberg wouldn’t be expected to know any more about science, medicine, or PCR than any other member of the general public. So why did the BBC send their chief political correspondent to a press conference on public health and not their chief science or health correspondent? And why did the PM choose her to ask the first question? But the BBC wasn’t alone. Six other correspondents from leading news outlets asked questions that day; all were chief political correspondents, none were science or health correspondents. So none of the journalists allowed to ask questions had the necessary knowledge to subject the PM and his Chief Scientific and Medical Officers to any degree of real scrutiny With the rise in the number of coronavirus ‘cases’ and ‘deaths’ reported on a daily basis and the Prime Minister’s solemn warning that “many more families, are going to lose loved ones before their time” filling the headlines the following morning, questioning what the numbers actually meant became more and more impossible. If the press and the public had forgotten the 2009 Swine flu panic, and those who helped calm it down had dropped their guard, those whose intention was to make a gain had learned their lesson.
 The Corona Crisis of 2020
Subject the Corona Crisis of 2020 to close scrutiny and it begins to look more like a carefully orchestrated advertising campaign for vaccine manufacturers than a genuine pandemic. But that scrutiny has been made impossible for all kinds of reasons. ‘Follow the money’ was once the epitome of investigative journalism, popularised in the movie of the Watergate scandal, ‘All The President’s Men’ which followed the money all the way to the top. Now following the money is called ‘Conspiracy Theory’ and is a sackable offence in journalism, if not yet in other professions. The idea that there may be real conspiracies to make false representations with the intention of making a gain or exposing others to a risk of loss has now been driven so far beyond the pale it’s literally unthinkable. If PCR has been tried by media in the court of public opinion, the case for the prosecution was demonised and dismissed at the outset and prohibited by emergency legislation soon after. The Last Best HopeThe last line of defence against false representation in both science and the media is the law. It’s no coincidence that Science and Law use similar methods and similar language. The foundations of the Scientific Method were laid by the Head of the Judiciary, the Lord Chancellor of England Sir Francis Bacon, in the Novum Organum, published exactly 400 years ago last year. Both are based on ‘laws,’ both rely on hard physical evidence or ‘facts,’ both explain the facts in terms of ‘theories,’ both test conflicting facts and theories in ‘trials’ and both reach verdicts through juries of peers. In science the peers are selected by the editorial boards of scientific publications. In law they’re selected by judges. In both law and science trials revolve around ‘empirical’ evidence or ‘facts’ – hard physical evidence that can be verified through the act of experiencing with our five senses of sight, sound, touch, smell and taste. But facts by themselves are not enough. They only ‘make sense’ when they are selected and organised into some kind of theory, narrative or story through which they can be interpreted and explained. But there’s more than one way to skin a cat, more than one way to interpret the facts and more than one side to every story. To reach a verdict on which one is true, theories have to be weighed against each other rationally to judge the ratios of how closely each interpretation fits the facts. Trial By LawThe ability of PCR to detect the genetic fingerprint of a virus is proven beyond reasonable doubt, but its ability to give a true representation of either the cause, severity or prevalence of a disease hasn’t. To say the jury is still out would be an understatement. The jury has yet to be convened and the case yet to be heard. Testing coronavirus particles in a swab is no different to testing apples in a bag. A bag of billiard balls rinsed in apple juice would test positive for apple DNA. Finding apple DNA in a bag doesn’t prove it contains real apples. If the dose makes the poison then it’s the quantity we need to test for, not just its genetic fingerprint. Grocers test the amount of apples in bags by weighing them on scales calibrated against standard weights. If the scales are properly calibrated the bag should weigh the same on any other set of scales. If it doesn’t, local trading standards officers test the grocer’s scales against standard weights and measures. If the scales fail the test the grocer can be prohibited from trading. If it turns out the grocer deliberately left the scales uncalibrated to make a gain they can be prosecuted for ‘false representation’ under section 2 of the Fraud Act 2006. Testing the quantity of viral DNA in a swab, not the quantity of live viruses, is like counting billiard balls rinsed in apple juice as real apples. Worse still, in the absence of standards to calibrate PCR tests against results, tests can show a “million-fold difference in viral load in the same sample.” If a grocer’s scales showed a million-fold difference in the load of apples in the same bag they’d be closed down in an instant. If it can be shown that the grocer knew the weight displayed on the scales may have been untrue or misleading, and they did it to make a gain or expose customers to a loss, it would be an open-and-shut case, done and dusted in minutes. If the law applies to the measurement of the quantity of apples in bags, why not to the measurement of coronavirus in clinical swabs? By the CDC’s own admission, in its instructions for use of PCR tests:
From that statement alone it’s clear that PCR tests may give a false representation that is untrue or misleading. If those using PCR tests to represent the number of Covid cases and deaths know it may be misleading and do it to ‘make a gain,’ either monetary or just to advance their own careers, it’s ‘fraud by false representation.’ If they have a duty to disclose information and they don’t do it it’s ‘fraud by failing to disclose information.’ And if they occupy positions where they’re expected not to act against the interests of the public but do it anyway it’s ‘fraud by abuse of position.’ If the law won’t prosecute those in authority for fraud, how else can they be discouraged from doing it? As Dr. Trish Perl said after the Dartmouth Hitchcock incident, “Pseudo-epidemics happen all the time. It’s a problem; we know it’s a problem. My guess is that what happened at Dartmouth is going to become more common.”The potential of PCR to cause problems will only get worse until its validity to diagnose the cause and measure the prevalence of a disease is tested in law. The last word on PCR belongs to its inventor, Kary Mullis: “The measurement for this is not exact at all. It’s not as good as our measurement for things like apples.” |
|
Why Is The CDC Quietly Abandoning The PCR Test For COVID?BY TYLER DURDEN 25July2021 https://www.zerohedge.com/covid-19/why-cdc-quietly-abandoning-pcr-test-covid We have detailed (most recently here and here) the controversy surrounding America’s COVID “casedemic” and the misleading results of the PCR test and its amplification procedure in great detail over the past few months.
As a reminder, “cycle thresholds” (Ct) are the level at which widely used polymerase chain reaction (PCR) test can detect a sample of the COVID-19 virus. The higher the number of cycles, the lower the amount of viral load in the sample; the lower the cycles, the more prevalent the virus was in the original sample. 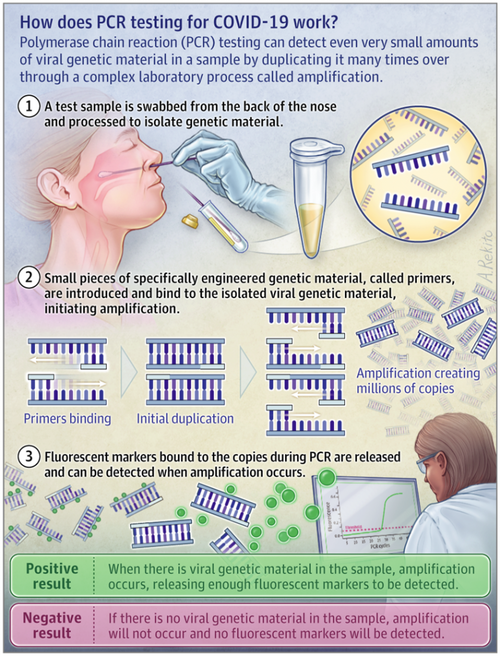 How does PCR testing for COVID-19 work?
Numerous epidemiological experts have argued that cycle thresholds are an important metric by which patients, the public, and policymakers can make more informed decisions about how infectious and/or sick an individual with a positive COVID-19 test might be. However, as JustTheNews reports, health departments across the country are failing to collect that data. Here are a few headlines from those experts and scientific studies:
So, in summary, with regard to our current “casedemic”, positive tests as they are counted today do not indicate a “case” of anything. They indicate that viral RNA was found in a nasal swab. It may be enough to make you sick, but according to the New York Times and their experts, probably won’t. And certainly not sufficient replication of the virus to make anyone else sick. But you will be sent home for ten days anyway, even if you never have a sniffle. And this is the number the media breathlessly reports… and is used to fearmonger mask mandates and lockdowns nationwide…
In October we first exposed how PCR Tests have misled officials worldwide into insanely authoritative reactions. As PJMedia’s Stacey Lennox wrote, the “casedemic” is the elevated number of cases we see nationwide because of a flaw in the PCR test. The number of times the sample is amplified, also called the cycle threshold (Ct), is too high.
A month later, Dr. Pascal Sacré, explained in great detail how all current propaganda on the COVID-19 pandemic is based on an assumption that is considered obvious, true and no longer questioned: Positive RT-PCR test means being sick with COVID. This assumption is misleading. Very few people, including doctors, understand how a PCR test works.
 Dr. Anthony Fauci In mid-November, none other than he who should not be questioned – Dr. Anthony Fauci – admitted that the PCR Test’s high Ct is misleading:
So, if anyone raises this discussion as a “conspiracy”, refer them to Dr.Fauci. In response to this and the actual “science”, Florida’s Department of Health (and signed off on by Florida’s Republican Governor Ron deSantis), decided that for the first time in the history of the pandemic, a state will require that all labs in the state report the critical “cycle threshold” level of every COVID-19 test they perform. Then, in January, as Biden takes office, The FDA publicly admits it…
First Fauci, then WHO, and then FDA all admit there is malarkey in the PCR Tests, but have – until now, done nothing about it… allowing the daily fearmongering of soaring “cases” to enable their most twisted 1984-esque controls. All of which brings us to today’s announcement from The FDA, that it will be abandoning the PCR Test for COVID at the end of the year.
The question one is forced to ask is simple – as with everything else that happens in the Healthcare-Industrial-Complex – cui bono? Is another provider of testing about to be enrichened? Or is it even more sinister than standard crony capitalism? Given the traditional winter spike in ‘flu’ cases and the PCR-Test-driven “casedemic” we experienced into the election and through the start of the Biden administration, one could be forgiven for suggesting that the last thing an already weakened Democratic Party, desperate to cling to control in DC, would be a dramatic re-emergence of the “deadly” virus (driven by the numerous false positives of the PCR Test as described in detail above) ahead of the Midterms? |
|
WHO (Finally) Admits PCR Tests Create False Positivesby Tyler Durden Sunday, December 20, 2020 – 8:12 https://www.zerohedge.com/medical/who-finally-admits-pcr-tests-create-false-positives Authored by Kit Knightly via Off-Guardian.org, Warnings concerning high CT value of tests are months too late…so why are they appearing now? The potential explanation is shockingly cynical…
The World Health Organization released a guidance memo on December 14th, warning that high cycle thresholds on PCR tests will result in false positives. While this information is accurate, it has also been available for months, so we must ask: why are they reporting it now? Is it to make it appear the vaccine works? The “gold standard” Sars-Cov-2 tests are based on polymerase chain reaction (PCR). PCR works by taking nucleotides – tiny fragments of DNA or RNA – and replicating them until they become something large enough to identify. The replication is done in cycles, with each cycle doubling the amount of genetic material. The number of cycles it takes to produce something identifiable is known as the “cycle threshold” or “CT value”. The higher the CT value, the less likely you are to be detecting anything significant. This new WHO memo states that using a high CT value to test for the presence of Sars-Cov-2 will result in false-positive results. To quote their own words [our emphasis]:
They go on to explain [again, our emphasis]:
Of course, none of this is news to anyone who has been paying attention. That PCR tests were easily manipulated and potentially highly inaccurate has been one of the oft-repeated battle cries of those of us opposing the “pandemic” narrative, and the policies it’s being used to sell. Many articles have been written about it, by many experts in the field, medical journalists and other researchers. It’s been commonly available knowledge, for months now, that any test using a CT value over 35 is potentially meaningless. Dr Kary Mullis, who won the Nobel Prize for inventing the PCR process, was clear that it wasn’t meant as a diagnostic tool, saying:
And, commenting on cycle thresholds, once said:
The MIQE guidelines for PCR use state:
This has all been public knowledge since the beginning of the lockdown. The Australian government’s own website admitted the tests were flawed, and a court in Portugal ruled they were not fit for purpose. Even Dr Anthony Fauci has publicly admitted that a cycle threshold over 35 is going to be detecting “dead nucleotides”, not a living virus. Despite all this, it is known that many labs around the world have been using PCR tests with CT values over 35, even into the low 40s. So why has the WHO finally decided to say this is wrong? What reason could they have for finally choosing to recognise this simple reality? The answer to that is potentially shockingly cynical: We have a vaccine now. We don’t need false positives anymore. Notionally, the system has produced its miracle cure. So, after everyone has been vaccinated, all the PCR tests being done will be done “under the new WHO guidelines”, and running only 25-30 cycles instead of 35+. Lo and behold, the number of “positive cases” will plummet, and we’ll have confirmation that our miracle vaccine works. After months of flooding the data pool with false positives, miscounting deaths “by accident”, adding “Covid19 related death” to every other death certificate…they can stop. The create-a-pandemic machine can be turned down to zero again. …as long as we all do as we’re told. Any signs of dissent – masses of people refusing the vaccine, for example – and the CT value can start to climb again, and they bring back their magical disease. |
|
FDA Recalls Millions Of At-Home COVID-19 Tests Over False Positivesby Tyler Durden 13November2021 – https://www.zerohedge.com/covid-19/fda-recalls-millions-home-covid-19-tests-over-false-positives Authored by Jack Phillips via The Epoch Times, The U.S. Food and Drug Administration (FDA) confirmed Thursday it is recalling some 2 million Ellume at-home COVID-19 testing because they can produce “false positives” due to a manufacturing defect.
The firm first informed the federal regulatory agency about the defect in some lots in October. But on Wednesday, the FDA said it identified additional lots that were affected by the manufacturing defect, made between Feb. 24, 2021, and Aug. 11, 2021. To date, about 35 false positives from the COVID-19 tests were reported to the FDA. No deaths have been reported related to the test, according to the agency. A “false positive” indicates that an individual has contracted the CCP (Chinese Communist Party) virus, which causes COVID-19, when they actually do not. The FDA noted that false positives could lead to “delayed diagnosis or treatment for the actual cause of the person’s illness, which could be another life-threatening disease that is not COVID-19” or receiving “unnecessary COVID-19 treatment from a health care provider,” which may “result in side effects.” Another problem, the FDA noted, is isolation, including monitoring household or close contacts for symptoms, limiting contact with family or friends, and missing school or work.” Underscoring the severity of the issue, the FDA said it “identified this as a Class I recall, the most serious type of recall … use of these tests may cause serious adverse health consequences or death.” The antigen test detects proteins from the CCP virus from a nasal sample, and it’s available without a prescription for use by people aged 2 years and older. It also comes with an analyzer that connects with a smartphone app to show users to perform the test and understand the test results. Ellume has recalled 2,212,335 tests in the United States to date. Earlier this year, the Australia-based firm announced it had about 200,000 of its tests. The Biden administration had signed a $231 million deal with Ellume, which received approval to produce its tests under the Trump administration last year. In October, Dr. Sean Parsons, Ellume’s chief executive, announced that the firm had created more safeguards to stop the problem from occurring again.
And a spokesperson said that the “root cause” of the issue was identified. The company is already shipping new products inside the United States, the spokesperson added to the NY Times. The Epoch Times has contacted Ellume for comment. |

New research shows that wearing a mask will not protect you against the coronavirusTuesday, November 24, 2020 by: Ethan Huff https://www.naturalnews.com/2020-11-24-wearing-mask-will-not-protect-you-against-covid19.html
(Natural News) Danish scientists finally found a journal brave enough to publish new research they compiled to show that mask-wearing is, at best, a placebo when it comes to protecting against the Wuhan coronavirus (COVID-19). Contrary to claims made by Anthony Fauci, establishment Democrats, and others that wearing a face mask is the most effective way to avoid infection, experts from across the pond discovered that covering up one’s mouth and nose does pretty much nothing to protect a person against the novel virus. Published in the Annals of Internal Medicine, the study looked at 4,862 participants, half of whom were instructed to wear a mask in public. The other half were instructed to go about their lives as normal breathing fresh air. Antibody testing conducted later on in the research revealed that 42 of the participants who wore a mask showed up as positive compared to 53 of those who did not wear a mask. The other 4,767 participants all tested negative, regardless of whether or not they wore a mask. Because the positivity rate between mask-wearers and non-mask-wearers was roughly equal at 1.8 percent and 2.1 percent, respectively, the researchers concluded that the difference was statistically insignificant – meaning masks cannot be scientifically shown to protect against the virus. “Our study gives an indication of how much you gain from wearing a mask,” stated lead author Dr. Henning Bundgaard. “Not a lot.” Dr. Christine Laine, Editor-in-Chief of the Annals of Internal Medicine, added a little more spin to the findings, suggesting that masks are “not a magic bullet.” The CDC on its website also explains that the “real-world” effectiveness of masks has not been scientifically proven, as any associated research is currently “limited to observational and epidemiological studies.” CDC journal declares face masks non-effective at preventing transmission of virusesIt apparently took a while to find a journal that was willing to publish these politically incorrect findings. Now that they have been published, the mainstream media is scrambling to come up with a response. The New York Times, for instance, is claiming that the study’s conclusion “flies in the face of other research suggesting that masks do protect the wearer,” though such research was not delineated. The Times went on to present statements made by the CDC in its latest bulletin claiming that cloth masks may – emphasis on the word may – help to protect the wearer. Whether or not they do for sure, however, has yet to be established. Desperate to maintain the pro-mask narrative, the Times went on to present various hypotheticals that could potentially negate the validity of these latest findings, such as participants not wearing their masks correctly. However, the journal Emerging Infectious Diseases, which just so happens to be published by the CDC, included a study of its own in the May 2020 edition that disagrees with the Times and actually validates this latest research out of Denmark. In that study’s abstract, scientists explain that after a review of various nonpharmaceutical personal protective measures and environmental hygiene measures as employed in various non-healthcare settings, a determination was made that face masks do “not support a substantial effect on transmission of laboratory-confirmed influenza.” “We similarly found limited evidence on the effectiveness of improved hygiene and environmental cleaning,” the paper adds. In other words, pretty much everything the “authorities” are now telling people to do, from profusely washing hands to wearing a mask at all times to constantly using hand sanitizer, is certifiably useless as far as actual science is concerned. “Disposable medical masks (also known as surgical masks) are loose-fitting devices that were designed to be worn by medical personnel to protect against accidental contamination of patient wounds, and to protect the wearer against splashes or sprays of bodily fluids,” the paper concluded. “Our systematic review found no significant effect of face masks on transmission of laboratory-confirmed influenza.” More of the latest news about COVID-19 can be found at Pandemic.news. Sources for this article include: |
|
COVID Lockdowns May Have No Clear Benefit vs Other Voluntary Measures, International Study ShowsBy Natalie Colarossi On 1/14/21 at 11:41 AM EST https://www.newsweek.com/covid-lockdowns-have-no-clear-benefit-vs-other-voluntary-measures-international-study-shows-1561656 A study evaluating COVID-19 responses around the world found that mandatory lockdown orders early in the pandemic may not provide significantly more benefits to slowing the spread of the disease than other voluntary measures, such as social distancing or travel reduction. The peer reviewed study was published in the European Journal of Clinical Investigation on January 5, and analyzed coronavirus case growth in 10 countries in early 2020. The study compared cases in England, France, Germany, Iran, Italy, Netherlands, Spain and the U.S. – all countries that implemented mandatory lockdown orders and business closures – to South Korea and Sweden, which instituted less severe, voluntary responses. It aimed to analyze the effect that less restrictive or more restrictive measures had on changing individual behavior and curbing the transmission of the virus. The researchers used a mathematical model to compare countries that did and did not enact more restrictive lockdown orders, and determined that there was “no clear, significant beneficial effect of [more restrictive measures] on case growth in any country.” “We do not question the role of all public health interventions, or of coordinated communications about the epidemic, but we fail to find an additional benefit of stay-at-home orders and business closures,” the research said. However, the researchers also acknowledged that the study had limitations, and noted that “cross-country comparisons are difficult,” since nations may have different rules, cultures, and relationships between their government and citizenry. The study was conducted by researchers affiliated with Stanford University, and was co-authored by Jay Bhattacharya, a professor of medicine and economics who has been a vocal opponent of coronavirus lockdowns since March. Bhattacharya was also among a group of scientists who wrote The Great Barrington Declaration, a controversial statement that encouraged governments to lift lockdown restrictions to achieve herd immunity among young and healthy people, while focusing protections on the elderly. … |
|
Big Pharma’s ‘Narrative’ Is Failingby Tyler Durden 09August2020 https://www.zerohedge.com/political/big-pharmas-narrative-failing Authored by Bretigne Shaffer via LewRockwell.com, So now we don’t have to listen to what those doctors said in front of the US Supreme Court, because it turns out that one of them has some whacky beliefs about sex with demons causing reproductive disorders. What a relief. I’m not going to pretend that the things Dr. Stella Immanuel has said don’t sound just a little crazy to me. They do. But I’ve been observing this game long enough to have a pretty good idea of how this works:
I understand that for some people, maybe even for a great many, that is the end of the conversation. So for everyone who is satisfied with the “fringe doctors promoting hydroxychloroquine also believe demon sex causes fybroids” narrative–please, stop here. Your ride is over, and you may go on believing that this group of doctors and other professionals has been thoroughly discredited by these statements. For everyone else, if you are at all interested in why such a coordinated effort has been launched to silence and discredit this group, why – even before the sex demon stuff was uncovered – videos of the group’s press conference were quickly yanked from YouTube, and why their own website was taken down without warning by its host, SquareSpace, (their new website can now be found here) then please keep reading. WHAT THE AMERICA’S FRONTLINE DOCTORS GROUP SAID:What follows is a brief summary of the key points made by the group America’s Frontline Doctors at their press conference last week. I will not comment on the validity of their claims, however founder Dr. Simone Gold has provided support for much of what the group said, in a white paper that can be found here. 1. They believe that hydroxychloroquine is an effective treatment for Covid-19.This is the claim made by several of the speakers, including Dr. Immanuel, based on their own clinical experience, as well as on multiple published studies. Many of those studies are listed here, and here. 2. State licensing boards are using their power to forcibly prevent people from having access to this drug.According to Dr. Gold, many states have empowered their pharmacists to not honor prescriptions for hydroxychloroquine to be used in treating Covid-19. This, she says, is unprecedented:
Meanwhile, says Gold, the drug is available over the counter in many other countries, including Iran and Indonesia, where it can be found “in the vitamin section”. 3. There is a coordinated campaign to discredit and suppress information about the drug hydroxychloroquine as a possible treatment for Covid-19:
Dr. Todaro is speaking from experience. He was the co-author of a March 13 white paper arguing for the use of hydroxychloroquine against Covid-19. The paper was made public on Google Docs, received a lot of attention, and was then removed–without warning–by Google. (It has since been put back up.) 4. The World Health Organization halted its trials of hydroxychloroquine based on a blatantly fraudulent study that relied on data that it appears never even existed.Bear in mind that this is the authority upon which YouTube CEO Susan Wojcicki has said she bases her company’s policy on “misinformation”. The WHO later resumed trials after independent investigators discovered the problems and the study’s authors retracted it. 5. We should be able to have a free and open discussion about this.Dr. Dr. Joseph Lapado from UCLA, sums it up:
WHY THE ALL-OUT MEDIA ASSAULT ON THE FRONTLINE DOCTORS?:The influence that the pharmaceutical industry wields over media outlets is no secret. As of 2018, an estimated 70% of all news advertising in the US came from pharmaceutical companies. I have written elsewhere about how “reporting” on medical issues can be difficult to distinguish from outright marketing for drug companies. Social-media platforms are not immune to this influence, whether it comes via advertising dollars; “partnerships” such as that between the CDC Foundation and MailChimp (which like many other platforms, has an explicit policy of censoring content about vaccines that does not align with the positions of the CDC and the WHO); direct investment, such as that of Google’s parent company Alphabet; or indeed at the behest of politicians such as Congressman Adam Schiff, who last year wrote to the CEOs of Amazon, Facebook and Google, requesting that those companies censor information and products that did not conform to the officially sanctioned position on vaccines. All three complied. So it should come as small surprise that both Google and YouTube have now taken to removing content supportive of hydroxychloroquine, a drug that is no longer covered by patent, and can be made and sold by any generic producer, for a fraction of the price that Gilead, for example, might charge for its still-patented Remdesivir. Twitter and Facebook have likewise removed posts about the drug, most notably–and with no visible sense of irony–removing posts of the video in which the Frontline Doctors speak out about widespread media censorship of the topic. (You can now see those videos on Bitchute.) One need not have an opinion on the merits of the drug hydroxychloroquine in order to recognize that something very odd is happening here. Something that doesn’t seem to have anything to do with free and open inquiry or honest scientific discourse. Many argue that the politicization of this drug is founded in a desire to unseat President Trump, that the opposition to it is primarily because it was endorsed by Trump, and if it is deemed to be a failure (or even better, dangerous to patients) it will be a powerful strike against the president. That may well be part of what has motivated this. But there is another motivation, having to do with the desire to push a more expensive medication onto the market, and to push a new vaccine on the world’s population. More broadly, it has to do with the narrative that those in the business of selling drugs demand we believe: that we are all in desperate need of their products (but only the ones still under patent) if we are to be healthy–or indeed, if we are to survive at all. If it turns out that this “new” virus is easily treatable, with hydroxychloroquine or anything else, then the industry’s dreams go up in smoke. If hydroxychloroquine turns out to be a safe and effective way of treating Covid-19 (as multiple studies and the experience in many other countries outside of the US indicate it may be) then there is much less reason for anyone to receive a vaccine for it, let alone the entire world’s population. Likewise, there is no pressing need to develop a new, more expensive treatment. But even more than that: If it turns out that hydroxychloroquine is after all a safe and effective treatment for Covid-19, then this whole episode – the silencing of dissenting voices, the “fact-checking” on social media, the campaigns against “misinformation” – will be revealed in plain sight, for what it has always been: Nothing more than a well-funded marketing campaign and damage-control effort on behalf of the industry that wants you to believe that you need to use its expensive products in order to go on living. So when a group of doctors took to the steps of the US Supreme Court and told the world how they were having success using a cheap anti-malarial that had been in use for 65 years to treat the most deadly contagion of our generation, it was a massive blow to the narrative upon which the pharmaceutical purveyors’ success depends. And over the next few days, as viewers engaged in a race with the censors, quickly downloading videos before they were removed, to post them on other platforms… it became clear that the censors and the gatekeepers had lost control of the conversation. This is not only about hydroxychloroquine. Every time media outlets or social-media platforms engage in outright censorship of content, in a way that happens to benefit pharmaceutical companies, both parties lose just a little more credibility. The actions we are witnessing now are not the actions of an industry confident in the value of what it provides to the world. They are the actions of a desperate, threatened creature. They are the actions of an entity that is not strengthened by the truth, but weakened by it. That is what these (increasingly obvious) acts of censorship tell us. What we are witnessing are the pangs of a lumbering, wounded, behemoth. The “Smoking Gun” study of why studies of Hydroxychloroquine to treat COVID-19 have failed. Hydroxychloroquine, evidence of efficacy |
|
Symptoms: COVID-19 vs. Cold or Flu | Do you have a Fever and a Dry Cough?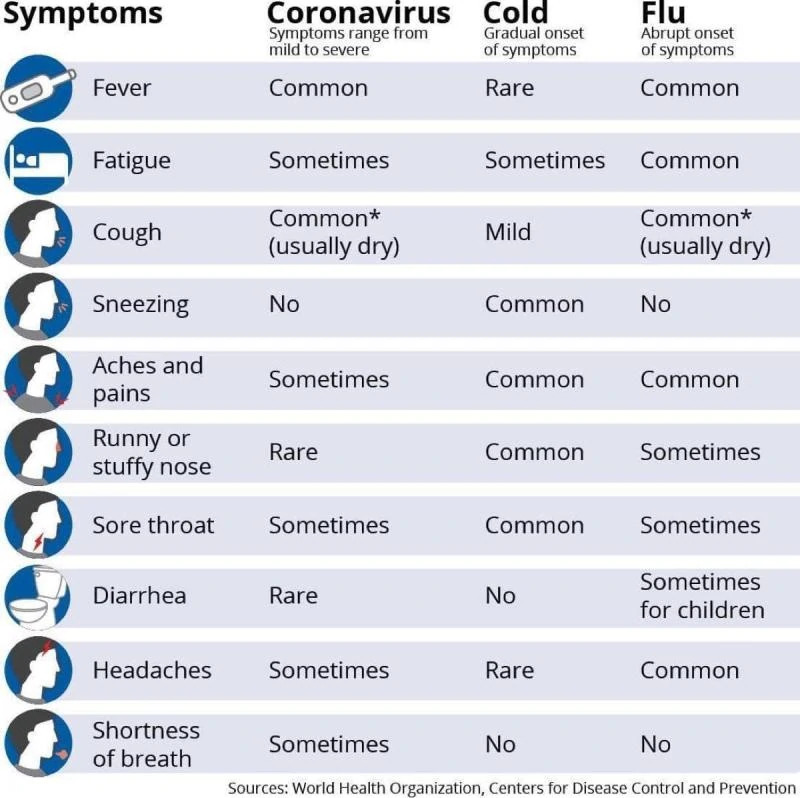 Symptoms: COVID-19 vs. Cold or Flu https://regenexx.com/blog/coronavirus-myths-debunked/ Aditional Symptoms: Loss of smell Loss of sense of smell as marker of COVID
 Coronavirus remains in the throat for four days. These are not the Symptoms of Coronavirus COVID-19: If you have these Symptoms It is time to get off your Apple iPhone or other Smartphone and go to bed.
Smartphone Zombies Approved by the World Health Organization from China: Coronavirus Quick Test | Chinese Fortune Cookie Approved by the World Health Organization from China: Coronavirus Quick Test | Chinese Fortune Cookie
|
|
Take Vitamin D and Zinc to prevent DeathQuite Compelling EvidenceDr. John Campbell 13May2020
Planning a randomized clinical trial, moderate to high doses In the meantime, |
|
The mortality rate for covid-19 is falling rapidly, and here’s how we can continue to improve it29September2020 by: Lance D Johnson https://www.naturalnews.com/2020-09-29-mortality-rate-for-covid-19-is-falling-rapidly.html (Natural News) In March 2020, the mortality rate for covid-19 was advertised as a scary 3.4 percent by the World Health Organization and experts such as Dr. Anthony Fauci. As more data was collected over time, the mortality rate fell. The latest numbers from the Centers for Disease Control (CDC) break down the mortality rate by age group. If an individual does become infected, the CDC has prepared a “current best estimate” of the mortality rate based on data collected from March through September and taking into consideration the R naught factor. The mortality rate for covid-19 should only concern those ages 70 and upBased on an R naught factor of 2.5, children between the ages of 1 and 19, if infected, are only at a .00003 risk of dying. The risk to schoolchildren is so low; schools should have never closed or implemented such strict behavioral controls. For young and middle-aged adults, ages 20 – 49, the risk of dying is still slight, approximately .0002. Almost every working age adult should be living their life as normal as possible, no longer controlled by arbitrary mandates. As with most infections, the risk of death appears slightly greater for those ages 50 to 69: The risk of death for those infected in this age group is .005. The only concerning mortality statistic is for people ages 70 and up. The mortality rate for infected individuals in this group is 1 in 20. Sadly, policies put forth by Governor Andrew Cuomo in New York forced positive covid-19 patients back into the nursing homes, putting the most vulnerable population at risk and driving up the mortality rate. How do we continue to lower the mortality rate?Improvements can be made to the mortality rate if every American started focusing on strengthening their immune system, instead of fearing their environment. Hydroxychloroquine (HCQ) and zinc should be made readily available to any patient with symptoms of a respiratory infection. Despite its effectiveness around the world, this treatment protocol has been suppressed and lied about, driving up the mortality rate. Zinc and SeleniumMedical researchers from the Leiden University Medical Center in the Netherlands found that the mineral zinc blocks viral replication for not only coronaviruses but all other RNA viruses, including poliovirus, respiratory syncytial virus, picornaviruses, and influenza viruses. Zinc works by correcting the proteolytic processing of viral poly-proteins. Zinc’s antiviral properties convey an up-regulation of interferon production, allowing the innate immune system to more rapidly respond to the virus to eliminate the infection from the body. Furthermore, zinc possesses anti-inflammatory activity and allows T-cell immune function to work efficiently, limiting cytokine storms that are observed in severe cases of covid-19. Other trace minerals are important for healthy immune function, including selenium. Vitamin DA study from Spain found that covid-19 patients respond well to vitamin D supplementation, even after infection. In the study, patients who tested positive for covid-19 were hospitalized 50 percent of the time when vitamin D was withheld. Two of the ICU patients did not survive. Another covid-19 positive group was given vitamin D. This group only saw one ICU admission (out of the 50 people studied) and that person did survive. Vitamin C and QuercetinA study titled, “Quercetin and Vitamin C: An Experimental Synergistic Therapy for the Prevention and Treatment of SARS-CoV-2 Related Disease (COVID-19)” found that quercetin interferes “at multiple steps of pathogen virulence,” including at “virus entry, virus replication, (and) protein assembly” to stop viral infection and proliferation. When quercetin is used in synergy with Vitamin C, the two become a prophylactic (preventative medicine) for the treatment of covid-19 and other respiratory tract infections. Licorice rootGlycyrrhiza glabra (licorice root) is one of many over-the-counter antiviral herbs that can be used to stop infections in the body. In vitro studies conducted on licorice root reveal antiviral activity against HIV?1, SARS related coronavirus, respiratory syncytial virus, arboviruses, vaccinia virus and vesicular stomatitis virus. Sweet wormwoodArtemisinin A is an active derivative of sweet wormwood herb (Artemisia annua /A. annua). This plant-based medicine inhibits SARS-CoV and other viruses in clinical studies. The plant’s concentration of aurantiamide acetate impedes cathepsin-L (CTSL), a protein that is critical for SARS-CoV-2 to gain entry into cells. Similar drugs are being developed to target CTSL to treat covid-19, and sweet wormwood herb provides the same medicinal mechanisms. To learn more on living with viruses and overcoming infections naturally, visit ImmuneSystem.News. Sources include: |
|
|
|
Rav Elyashiv, the Vilna Gaon’s Lottery and CoronavirusBy Josh Wander 4 Nisan 5780 – 29March2020 https://www.jewishpress.com/news/israel/aliyah-israel/rav-elyashiv-the-vilna-gaons-lottery-and-coronavirus/2020/03/29/ גורל הגרא על נגיף הקורונה הרב בנימין אלישיבmyinternetfavs 25March2020 There is a ancient Jewish tradition, that in more modern times is attributed to the Vilna Gaon, called the “Goral HaGra”. It is a lottery which is done at times of extreme need. When divine assistance in required to answer a question of national significance. Great rabbis have passed down this tradition, which allows for a query to be made via a specific protocol and then a Chumash is opened to a random page and a Pasuk is pointed to. This verse is understood to be the answer to the query that was posed. It was used during the Holocaust to determine in which direction the Mir Yeshiva should escape to (eventually leading them to Shanghai) and again by Rav Aryeh Levin z”l to identify the remains of the mass grave of Jews killed in the Old City of Jerusalem during the War of Independence. There are very few rabbis alive today who are knowledgeable and qualified to conduct this ceremony. But it was performed this past week in Jerusalem by none other than Rav Aryeh Levin’s grandson and son of the famous Posek, Rav Binyamin Elyashiv Shlit”a. Rav Binyamin Elyashiv is recognized as one of the poskim, leading Halachic deciders, in the Haredi community in Israel today. Rav Elyashiv was asked by a American Jewish supporter of Torah institutions how they should be responding to the CoronaVirus in this time of crisis and whether they should relocate to Israel. The response received by the divine lottery was nothing less than miraculous. The verse that was chosen came from Deuteronomy 1:8, where it states, “See, I have set the land before you; come and possess the land which the Lord swore to your forefathers, to Abraham, to Isaac, and to Jacob, to give them and their descendants after them.” This led the holy rabbi to explain to his grandson that this is a revelation and a clear sign that it is time for world Jewry to make their way back to the Land of Israel. “Israel is the safest place for a Jew to be now,” the rabbi said, “We are very close to the final redemption. It will all be over very soon here.” He also said that those who are left outside of the Land, but continue to support her, will also be recognized as being native to the land. JerusalemCats Comments: For All those that state “I will make Aliyah when Moshiach comes” Well Rav Zissholtz: 2 Geula Statements Heard Recently29March2020 http://yeranenyaakov.blogspot.com/2020/03/rav-zissholtz-2-geula-statements-heard.html (h/t Sod1820) Rav Zissholtz on Radio 2000 said the following (paraphrased):
|
|

Amsterdam: Jewish community in great distressDutch authorities refusing to allow Jewish community to aid elderly coronavirus victims, Amsterdam rabbis say.Yoni Kempinski , 08May2020 http://www.israelnationalnews.com/News/News.aspx/279913 Amsterdam Rabbi Eliezer Wolff and former Amsterdam Chief Rabbi Aryeh Ralbag spoke about how Holland’s healthcare system is failing to treat elderly coronavirus patients. In a Zoom conference with the Conference of European Rabbis (CER), the two described the health authorities’ attitude towards coronavirus patients over 60 years of age. “They don’t provide medical aid, certainly not ventilators, and to our great sorrow we have again seen actual opposition, even in the Jewish nursing home. They don’t evacuate patients who require hospitalization, and since we were called in to help, unfortunately, we have lost another four elderly. They also speed up their deaths, by giving them high doses of morphine,” the two said. Dutch authorities rejected the CER’s offer to pay to hire a special doctor and purchase ventilators for the Jewish community. Baruch Van De Kamp, one of the community’s more wealthy members, suggested allocating one of his hotels for the isolation of elderly patients who contracted coronavirus, but this suggestion was also rejected. “It’s extremely saddening to hear that specifically a country considered to be ‘progressive’ is insensitive to the value of life and even determinedly refuses any aid offered by others, Moscow’s rabbi and CER President Rabbi Pinchas Goldschmidt said. The rabbis have decided to speak to the leaders of the community and the nursing home, expressing their sharp protest, and to declare that they will use any means available to them, if they are not allowed to aid the elderly patients. Later in the meeting, Rabbi Ralbag discussed the CER’s court in Amsterdam for women whose husbands refused to grant them a divorce, and the unprecedented ruling of the Dutch court: to arrest one of the divorce-refusing husbands for six months, due to his refusal to appear in the Jewish court. “Even though he is not a resident of Holland, the court issued an arrest warrant for him, allowing any country which is a member of the European Union to enforce it,” he said. |
|
It’s time to come home! Nefesh B’Nefesh: Live the Dream 1-866-4-ALIYAH UK 0800 075 7200 Come home to the Land of Emuna Nefesh B’Nefesh: Live the Dream US & CAN 1-866-4-ALIYAH | UK 020-8150-6690 or 0800-085-2105 | Israel 02-659-5800 https://www.nbn.org.il/ info@nbn.org.il Religious Jews are among the biggest victims of COVID-1929March2020 Elder of Ziyon http://elderofziyon.blogspot.com/2020/03/religious-jews-are-among-biggest.html 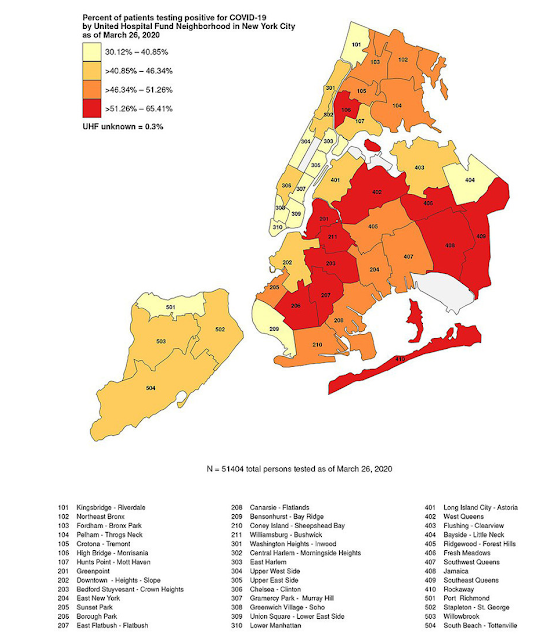 Religious Jews are among the biggest victims of COVID-19
Boro Park. Flatbush. Crown Heights. Forest Hills. Fresh Meadows. Every single New York neighborhood with a large religious Jewish population has the highest percentage of patients testing positive for the coronavirus, according to this map published by the NYC Department of Health. Looking at New York State as a whole, the heavily Jewish Rockland County has a higher percentage of COVID-19 cases per capita than New York City (as far as I can tell, second only to Westchester County.) And in New Jersey, the two towns with the highest number of COVID-19 cases are not the major cities of Newark (155) or Jersey City (130) or Camden (2) or Trenton (7). They are the much smaller towns with large Jewish populations: Teaneck (population 37,000, Jews 15,000, 213 cases) and Lakewood (population 102,000, Jews 60,000, 198 cases.) Even though Orthodox rabbis across the board closed down all schools and synagogues before the government authorities said to, the sheer amount of interaction that religious Jews have with their communities – often going to prayer services 2 or 3 times a day, and this year especially celebrating Purim (March 10) together with friends and family, made Orthodox Jewish communities Ground Zero for the coronavirus. This was not helped by the refusal of a small minority to shut down their synagogues and cancel wedding parties – stupid, selfish decisions that are ensuring that the numbers continue to grow as we approach the two week mark since rabbis first called for the shutdowns. There were reports that some Jews still insisted on praying with others as recently as Friday. Only this week will we begin find out the effectiveness of the shutdowns that started on March 12 in Teaneck/Bergen County and then spread across the region in the following week. Every day we learn about more and more people we know, or in our circles, who have gotten ill or passed away. Often they are community leaders – rabbis and others – whose jobs involve close interaction with their followers. It is a very scary time, and the worst is still to come. We are facing a Passover without extended family. But it is necessary to keep all of our extended families as safe as possible. And those who continue to pretend to be “frummer” by still praying with a minyan/quorum are playing Russian roulette with their families, and everyone else’s lives. |
|
|
Brooklyn Hatzola issues dire coronavirus warning: ‘This is a crisis’By Gabrielle Fonrouge 19March2020 https://nypost.com/2020/03/19/brooklyn-hatzola-issues-dire-coronavirus-warning-this-is-a-crisis/ As the number of people infected with coronavirus continued to soar in the Orthodox Jewish community Thursday, Hatzola leaders warned that things must change before it’s too late. Borough Park’s Hatzola, an emergency ambulance service catering to the Jewish community, sent an urgent robocall across the neighborhood Thursday afternoon, a day after two urgent cares in the area reported an alarming spike in positive coronavirus cases. “It seems that in our community of Borough Park, life is continuing as normal, business as usual. People are going about their daily lives as if nothing is happening,” the recording says. “Many, many, many of our friends and family have contracted this virus and are not doing as well as we had hoped. This is a crisis… We need to do what’s right. And to the current moment, we have not done [that], we have not stepped up to the plate.” On Thursday morning, Asisa Urgent Care said they had around 400 positive cases come out of their two Borough Park facilities and Williamsburg location, accounting for nearly half of Brooklyn’s 1,030 infections reported by City Hall. That’s up from about 150 from the day before. The health care facility’s rep said about 99 percent of those tested were from the Jewish Orthodox community. The Hatzola call to action implored members of the community to heed the advice of doctors and “stop mingling.” “We must be more mindful of what’s happening and how we can stop the spread of this virus. We need to do more. We have done very little currently. We need to keep away from each other. We can’t stand next to each other. We have to protect each other as if we’re all fighting for our lives. This is no laughing matter,” the recording says. “If we are not going to be taking this seriously, who knows who will be there to help us?” During a press briefing late Thursday, Mayor Bill de Blasio insisted again there is “no cluster” of COVID-19 in Borough Park and said “that part of Brooklyn is not any more endangered than anywhere else.” Additional reporting by Julia Marsh |
|
In the shadow of the Coronavirus epidemic
Dear Diaspora RabbisThis is not the time for well-meaning Internet messages and sermons about unity in times of trouble, nor about the renewal of Diaspora life when the epidemic has passed.Tzvi Fishman 04April2020 http://www.israelnationalnews.com/Articles/Article.aspx/25493
Dear Diaspora Rabbis. In the shadow of the Coronavirus epidemic, with love and concern for you and your communities, now that your synagogues are closed, on behalf of myriads of Jews in Israel, many of them olim from the Diaspora, we bid you to reach out to your congregants via the Internet and telephone, and urge them to make Aliyah now. The gates are fast closing, but it is not too late. The Jewish Agency and Aliyah organizations like Nefesh B’Nefesh are still working. Just as the Government of Israel is endeavoring around the clock to return touring Israelis from around the world on emergency rescue flights, the State of Israel will do the same for you and your congregants if you act today. Now is not the time for procrastination and doubts. As Rabbi Kook once told a Jewish visitor to Israel, in order to free himself from the quagmire of the exile, a person must slay all extraneous excuses and not make an accounting (Heb. “Heshbone), just like the Jews exiting Egypt had to slay the King of Heshbone (name of king mentioned in the Bible) before entering the Promised Land. This is not the time for well-meaning Internet messages and sermons about unity in times of trouble, nor about the renewal of Diaspora life when the epidemic has passed. It is time to get out forever. If such an immediate relocation is too difficult for the aged, at the very least, all young Jews must be told the truth. Let them pack up a backpack and flee. Families in the Diaspora – don’t hold onto your children! Think about their futures, not about yourselves. Already around the world, looting and violence have begun. First stores will be vandalized when people have no money and food. In several places, the Jews have already been blamed for the plague. Just as the virus spread suddenly before it could be stopped, Jew hatred will explode like a fiery cloud of gas, scorching everyone in its wake. Overnight, masses will turn into savage skinheads and neo-Nazis. Hordes of desperate and wild packs will attack like rabid dogs. Jews and other innocents will be mugged, houses will be broken into, people will be shot, like in previous times. In Europe, hungry minorities will turn into rampaging gangs. In many places, the governments will look on silently as Jews are attacked, claiming that there is nothing they can do. In other places, like America, the authorities will not have the manpower to prevent the anarchy. There are complaints from patients in New York hospitals that aides are not entering rooms with Jews. The time to flee was years ago, but if not now, when? Experts are predicting that the evil could rage for months and more. At the very least, let the young people go! Rabbis, parents, if you love them, command them to flee! Let the cry be, “This year in Jerusalem!” If not, for a ghastly number, Passover will not come again, and homes of Jews will be passed over in a different, opposite sense, may the Almighty have mercy. The exile was never meant to last forever. Hashem meant the exile to be a curse, but, beaten down by the long oppression, we turned it into the illusion of having found havens of welcome and peace. The word of the Almighty is not a whimsical thing that can change with our fancies. He decreed the curse of exile, and He decreed that His outcast and scattered children would one day return. That time came with the founding of the Jewish State. For those who didn’t hear the call, or who refused to listen, the call of Corona, the virus of the Crown, of Hashem’s Kingship, is clear. Let it be the great shofar of our freedom. Now! There is a refuge in Israel, as our prophets foretold. Yes, we have problems. Yes, the virus is here as well. But the State of Israel reacted quickly to the threat. Every effort is being made to protect the Jewish people and overcome the enemy. In Israel, you will be amongst fellow Jews, with Jewish policemen and a Jewish army, and not at the mercy of strangers. Rabbis, Jewish educators, Federation presidents, and leaders of Jewish organizations – send the Jews to Israel! Teach by example! Show the way! Break through the sea of indecision and fear. We are waiting on the other side of the ocean to welcome you. Be brave like Nachshon. Leap into the waters of faith. Come home now! |


JerusalemCats Comments: Just look at the Tweet from March 31, 2020 of all the stores boarded up!
 Thousands of stores in New York have boarded up their doors and windows to avoid possible looting TRT World @trtworld tweet 31March2020
|
|
The Aliya Apocalypse is comingThe difference between the situation of Jews in the Diaspora and those in Israel during the corona pandemic has led to a change in the way Diaspora Jews look at the Jewish state, from the Zionists to the haredim to the progressives.Rabbi Elchanan Poupko 20April2020 http://www.israelnationalnews.com/Articles/Article.aspx/25567
 Aliyah landing
If there is one thing we know about the post-coronavirus era that connects with the post WWII eraa, it is that we have no idea what the world will look like.. Who will be the winners? Who will be the losers? We do not know what industries will survive and which won’t, which economies will rise, and which will crumble. As many have noted, for American Jews, the notion that America is a first-world country, and Israel is some kind of second world country can no longer exist. Sitting in New York hearing the harrowing sounds of ambulances all day and all night, while watching videos of Israelis singing Ma Nishtana from their balconies, can never be erased. The far superior management of the coronavirus outbreak in Israel, while we felt stranded and abandoned by state policies, will never disappear. Haredi Jews in Brooklyn and Rockland County who had seen tens of deaths a day for the past few weeks will never again be able to look down on Israel. The contrast between the swift and effective action taken in Israel confronting the coronavirus, although it did suffer fatalities – a much lower number proportionately than outside Israel – contrasted with the slow and inadequate actions taken against it in most states in America, highlights the technological, governmental, and medical superiority Israel has been able to exercise in defense of its citizens. This is something everyone considering making Aliya will now have on their minds. This is not true only of Jews in America. It is also true of Jews in the United Kingdom, France, Italy, Spain, Germany, Australia, and more. Then comes the economic aspect. We do not know when economies will go back to function. We do know that many aspects of the economy may never come back. Others will be very hard hit. We do know that the world may be facing the greatest economic depression since the 1930s. For American Jews it’s a simple choice: would you like to stay here to find out what a full-blown economic catastrophe looks like during an unresolved pandemic, with no guarantee for health insurance, not able to afford your children’s education, or would you like to take your chances and go to Israel? In Israel, you are guaranteed almost free healthcare—which has proven itself far superior and more effective—free or low-cost high-quality Jewish education (and low-cost higher education), and effective public policy (albeit with a civic license to complain and insane politics). It is hard to imagine this will be a difficult choice. Once the airways reopen, and a ravaged world economy emerges, it is likely we will see an Aliya apocalypse. Americans from all walks of life are likely to find the fast track back to Israel. Another group that is likely to find their way back are Israeli yordim, those who emigrated to other countries. Many of them decided to take a risk and relocate so they could succeed at building a better standard of life in New York, Florida, Berlin, or Los Angeles. When economic opportunities are at a one hundred year low, when they are guaranteed a better healthcare system, when the world is far less globalized than ever before, many of them are likely to jump on the first flight back to Israel available to them. Many have already.
Another change we are likely to see in Israeli-Diaspora relations is between the haredi sector and Israel. My heart bleeds as I think of the dozens who died and die every day in Brooklyn, Rockland County, Lakewood, Kiryas Joel, and more. Every day I turn with horror to the various sites to see if there is anyone I know, a family member, a friend, or a known community leader. Sadly, this happens almost every day and I hope is on a downward trend. I vividly recall standing in my home in New York, at the epicenter of the coronavirus outbreak, getting one of the usual charity calls from Israel. “You know the situation here is very difficult,” was the pitch. I couldn’t even pretend to listen. Hundreds of people were dying in New York and they were asking for sympathy? Thank G-d, they did not need it as much as we do! American Jews will realize that not being the big brother—benevolent uncle Sam—is not much fun. Earlier this year, Rav Ahron, one of the two current Satmar Rebbes, came from Brooklyn to Israel, greeted by thousands, donating five million dollars to non-Zionist institutions. There was a subtle message about his arrival. The drones on the way to the airport, the private jets, the fancy motorcades, dashing out cash to supporters, all gave a simple message: American dollars can outdo Zionism. Rabbi Mordechai Berkovitch, a leading figure in the Satmar community in America, said it then outright: “the Zionists bought the Jews of Israel for a few dollars, we are going to get them back with millions of dollars. We are going to fight them face to face.” If indeed this was a battle between the Brooklyn dollar and the Israeli Shekel, the outcome is not looking great for Brooklyn. Time to begin opting for Jerusalem over a beleaguered Brooklyn. This symbolism is not just true for Brooklyn. Jews in haredi communities in London, Manchester, and beyond will do the same. It is hard to imagine Jewish communities like Antwerp, Belgium, which are now bracing an 85% coronavirus infection rate, soon forgetting how much better off their cousins in Israel were during this period. Israel will become a far more appealing option than ever before. Progressive Jews won’t fall far behind either. Especially young ones. Reflecting on my days of hitting the job market during the 2008 recession, I can say with certainty there is nothing exciting about hitting a job market in decline. No matter what you think about Netanyahu, he did not abandon his citizens during the coronavirus outbreak just because they didn’t vote for him. Those who lived in blue states during this outbreak felt, although unjustifiably, abandoned and stranded by the federal government. The possibility of a country with nationalized healthcare, effective public health systems, an economy that is open both to the West and the East, is likely to appeal to many young Jews. During this coronavirus outbreak, we should be thinking about our friends, family, grandparents, and members of our community. We should be thinking about how to get over this 21st century horror alive and well, care for others, and look out for anyone we can. Israel has done so in a spectacular way. For that reason, Israel should also be preparing for the Aliya Apocalypse. Once the airways are open, many Jews will be saying: this year in Jerusalem. Israel should prepare to embrace them.
|
|
The roles have reversed with the US and Israel! Now Israel is providing the volunteers to aid the US. It is time for US Jews to make Aliyah before it is to late.
Israeli NGO Steps Up to Help Americans in Time of Need During Coronavirus Pandemicby Gary Shapiro 22April2020 https://www.algemeiner.com/2020/04/22/israeli-ngo-steps-up-to-help-americans-in-time-of-need-during-coronavirus-pandemic/ Twenty-two-year-old Amir Kashfi arrives early in the morning around 6:30 a.m. outside a Los Angeles school to set up boxes of canned goods, pasta, rice and other non-perishables to dispense. A number of recipients line up by car or by foot by 8 a.m. The need for this food pantry has spiked during the ongoing coronavirus crisis. “There’s a huge increase in demand because of the pandemic,” said Kashfi, a volunteer with IsraAID, an Israel-based NGO that partners with Los Angeles Regional Food Bank and Team Rubicon, which is a US veterans organization, among others in these efforts. “It hurts my heart to see so many in need.” “Our goal is to be there for the community,” said Seth Davis, chief executive officer of IsraAID US. He noted that the short-term goal was to fill a gap and get food to people in need, but the long-term goal was to create a cadre in the community who can respond to such crises. In addition to Los Angeles, IsraAID has helped operate food banks in other California locations, including San Diego, Orange County, San Jose and Santa Barbara. Davis said, “This deployment will go on for months, because even if the curve flattens, there’s going to be a long tail of people still in need of food and financial help.” “These are unprecedented times,” Dr. Lucy Uber, another volunteer, said. “Food is a basic necessity that most of us take for granted.” She reflected on the precariousness that many were experiencing at the moment. “Many of these people live in what is already referred to as a food desert,” said Uber. “Add the coronavirus crisis and there is financial devastation.” For her employment, not as a volunteer, she works in the emergency room at Children’s Hospital Los Angeles. Uber said, “The full socioeconomic impact of the coronavirus crisis may not be known for years.” The pediatrician Uber connected with IsraAID through a classmate from high school, Farah Shamolian, who works for IsraAID. “I went into medicine because I wanted to help people,” Uber said. After Uber attended medical school in Tel Aviv, she said, “I wanted to keep Israel close to my heart.” She is also part of the IsraAID Humanitarian Professionals Network, a collective of doctors, nurses, pharmacists, psychologists and others involved in humanitarian relief and disaster response. Uber said, “Its goal is to educate and motivate people to be ready to respond to crises abroad and locally.” In 2018, IsraAID deployed Kashfi to Berlin where he worked with Farsi-speaking refugees from Afghanistan, Iran and Tajikistan, as well Arab refugees from Iraq and Syria. Kashfi said, “It was not lost on me that I’m a Persian Jewish kid from Los Angeles helping Arab and Muslim refugees through an Israeli organization in a country where the Holocaust happened. You can’t make that up.” IsraAid, which has worked in 52 countries worldwide, has helped the US in crises before. In 2005, IsraAID assisted those in the path of Hurricane Katrina. It also sent a team in 2012 to help with Superstorm Sandy recovery efforts. It has responded to Hurricane Harvey in Texas, Hurricane Michael in Florida and Hurricane Florence in the Carolinas. They were also responders to the more recent fire of Paradise, California, working with local community leaders and caregivers to deal with the trauma. IsraAID is currently speaking with potential partners in helping New York state’s response to COVID-19. The organization already had a satellite office in New York. What might the focus be? Davis said, “People put a lot of focus on protective gear, the physical injury and the loss of life, but people are not putting enough focus on mental health and the emotional injury.” He added, “We don’t want people to get PTSD, but to have PTG or post-traumatic growth. We can build our skill set that caregivers, religious leaders and people in education have to help people bounce back stronger.” Davis said part of the focus will be on helping children, educators and healthcare professionals. IsraAID is not limited to the physical world in its efforts to assist. It also is helping in the virtual world. For, IsraAID designed a free online webinar to offer mental health support to those who experienced trauma during the COVID-19 crisis. It offers 12 practical ways to reduce anxiety and stress. It was devised in Israel at the headquarters of IsraAID by mental health and protection professionals. The volunteer Kashfi said, “IsraAID is not religious or political. It is a professional humanitarian organization. It’s a welcome side effect that our work reflects the values of Israel in a positive light.” |
|
Pesach Seder: Protect your Grandparents
 Arsen-strovsky-tweet-30March2020 Powerful message from @naftalibennett to Jewish communities around the world ahead of #Pesach: “Do the Pesach Seder in the very nuclear family. You do not do it this year with grandma and grandpa. There will be no Pesach Seder with young people and old people.”
|
Eating a plant-based diet can help protect against COVID-19, researchers find01August2021 by: Divina Ramirez https://www.naturalnews.com/2021-08-01-plant-based-diet-protects-against-covid-19.html  Veggies Vegetables Nutrition Healthy Diet Greens (Natural News) People who eat a plant-based diet are less likely to contract COVID-19 and become severely ill with the disease, according to a recent study by researchers from Harvard Medical School, King’s College London and the health science company ZOE. The researchers analyzed data from over 590,000 people from the United States and the United Kingdom who answered a survey about the foods they ate last February using the ZOE COVID Symptom Study application. The application allows users to record their symptoms in case of COVID-19 infection and to log when they’ve had a positive polymerase chain reaction (PCR) test. By early December 2020, 19 percent of the users who participated contracted COVID-19 based on positive PCR test results and symptoms reported via the application. “For the first time, we’ve been able to show that a healthier diet can cut the chances of developing [COVID-19],” said co-author Sarah Berry, a senior lecturer in nutritional sciences at King’s College London. A preprint of the study was released online in medRxiv. Eat more plant-based foods to avoid COVID-19Poor metabolic health and certain lifestyle factors are associated with an increased risk and severity of COVID-19, but data for diets are lacking. For their study, the researchers sought to analyze the association of diet quality with the risk and severity of COVID-19 and how that intersects with socioeconomic factors. To that end, the researchers examined data from 592,571 users of the ZOE COVID Symptom Study application from the U.S. and the U.K. The users completed a survey about the foods they ate in February 2020. The researchers scored users’ diet quality based on a scale that emphasized healthy, plant-based foods. The users were followed until December 2020 and asked to log if they had contracted COVID-19 or were hospitalized because of it. Diets with high quality scores were found to contain more plant-based foods, especially fruits, vegetables, nuts and whole grains. On average, people with high-scoring diets ate two pieces of fruit and three different vegetables per day. They also ate 200 grams (g) of fatty fish every week and limited their intake of refined grains and processed foods. People who eat plant-based foods have healthy microbes in their guts, said Tim Spector, a co-author of the study and a co-founder of ZOE. Having healthy gut microbes has been linked to better health. On the other hand, low-scoring diets were found to contain more processed foods. On average, users with low-scoring diets ate fewer than two pieces of fruit per week and went some days without eating any vegetable or oily fish. In addition, the researchers found that there were 72 cases of COVID-19 for every 10,000 person-months among users with high-scoring diets. Meanwhile, there were 95 cases of COVID-19 for every 10,000 person-months among users with low-scoring diets. Overall, the researchers found that users with high-scoring diets were 10 percent less likely to contract COVID-19 and 40 percent less likely to become severely ill with the disease than users with low-scoring diets. They estimated that nearly a quarter of users who became infected with COVID-19 could have avoided the disease if they ate a healthier diet. They also noted that users living in areas where plant-based foods were less available may face a greater risk of COVID-19 infection than users with easier access to those foods. How to get started on a plant-based dietThere is no need to go vegan to reap the health benefits of eating plant-based foods. Many healthy plant-based diets, such as the Mediterranean diet, still allow meats and animal products to a certain degree. However, you’re encouraged to limit your intake of those foods as much as possible. If you want to get started on a plant-based diet, keep the following tips in mind:
Fresh.news has more articles on the health benefits of eating plant-based foods. Sources include:
How eating your five-a-day may spare you from Covid: People who consume plenty of fruit and vegetables and cut out processed foods ‘are up to 40% less likely to fall severely ill with virus’
By Luke Andrews Health Reporter For Mailonline Published: 13July2021 https://www.dailymail.co.uk/news/article-9783301/People-eat-three-fruit-vegetables-day-40-likely-fall-severely-ill-virus.html
King’s College London experts asked 600,000 people to log what they were eating before the pandemic began.
Volunteers were divided into five groups based on how healthy their diets were.
They were also tracked for nine months and asked to tell researchers if they caught the coronavirus and log how ill they became.
Results showed those who ate the most greens were 40 per cent less likely to be hospitalised and need oxygen if they were infected.
And they were 10 per cent less likely to catch the virus in the first place.
The researchers defined the healthiest eaters as those who ate two pieces of fruit a day and three different vegetables.
They also had 200g of oily fish such as salmon and sardines every week and kept fatty and sugary processed foods to a minimum.
On the other hand, the unhealthiest eaters had fewer than two bits of fruit over the course of a week and went some days without eating any vegetables.
They also steered clear of oily fish, and consumed more fatty and sugary processed foods than recommended.
Professor Tim Spector, one of the researchers, said there was ‘no need to go vegan’ to reap the benefits of healthy eating.
But he said eating a more plant-laden diet could ‘improve your immune system’ and ‘potentially reduce your risk from Covid’.
Professor Spector said: ‘People who eat higher quality diets (with low levels of ultra-processed foods) have a healthier collection of microbes in their guts, which is linked to better health.’
Study co-author Dr Sarah Berry said: ‘For the first time we’ve been able to show that a healthier diet can cut the chances of developing Covid.’
The study was run through health-tech firm ZOE’s Covid Symptom Study app, which has been downloaded more than a million times.
The software — which allows people to log their symptoms and whether they had a positive test — is used to track the coronavirus outbreak in Britain.
Academics used data from more than 31,000 participants who were thought to have caught Covid across the UK and US.
Only a quarter actually tested positive for the virus — the rest were assumed to have been infected based on the symptoms they showed.
At the start of the pandemic there was a lack of tests available, leading to millions of cases being missed officially.
Participants were asked about what they ate in February last year, before the virus took hold.
They were followed until early December — through the first wave and the start of the second wave — and asked to log if they had the virus, or were hospitalised.
Data showed there were 72.2 cases of Covid for every 10,000 person-months among participants with the healthiest diets.
But for volunteers at the other end of the dietary spectrum, the rate stood at around 95.4.
The difference was even worse for cases of severe illness — defined as patients who were admitted to hospital and required oxygen.
After analysing the results for other potential factors that may have skewed the findings such as sex, ethnicity and underlying health conditions, they found those with the best diets were 40 per cent less likely to suffer severe disease and 10 per cent likely to catch the virus in the first place.
The study, which was published on medRxiv, also involved scientists from Harvard Medical School.
|
|
Authoritarianism In The Age Of Pseudoscienceby Tyler Durden 09May2020 https://www.zerohedge.com/health/authoritarianism-age-pseudoscience Authored by Colin Todhunter via Off-Guardian.org, Following the court decision in the US to award in favour of Dewayne Johnson (exposure to Monsanto’s Roundup weed killer and its active ingredient, glyphosate, caused Johnson to develop non-Hodgkin lymphoma), attorney Robert Kennedy Jr said at the post-trial press conference:
Johnson’s lawyers argued over the course of the month-long trial in 2018 that Monsanto had “fought science” for years and targeted academics who spoke up about possible health risks of the herbicide product.
 Monsanto Roundup sign near crops
Long before the Johnson case, critics of Monsanto were already aware of the practices the company had engaged in for decades to undermine science. At the same time, Monsanto and its lobbyists had called anyone who questioned the company’s ‘science’ as engaging in pseudoscience and labelled them ‘anti-science’. We need look no further than the current coronavirus issue to understand how vested interests are set to profit by spinning the crisis a certain way and how questionable science is again being used to pursue policies that are essentially ‘unscientific’ – governments, the police and the corporate media have become the arbiters of ‘truth’. Health Ranger DECLARES: End the LOCKDOWNS; launch the TAKEDOWNSHealth Ranger Report 07May2020
 What directions to go with science
We also see anyone challenging the policies and the ‘science’ being censored on social media or not being given a platform on TV and accused of engaging in ‘misinformation’. It’s the same old playbook. The case-fatality ratio for COVID-19 is so low as to make the lockdown response wholly disproportionate. Yet we are asked to blindly accept government narratives and the policies based on them. Making an entire country go home and stay home has immense, incalculable costs in terms of well-being and livelihoods. This itself has created a pervasive sense of panic and crisis and is largely a result of the measures taken against the ‘pandemic’ and not of the virus itself. Certain epidemiologists have said there is very little sturdy evidence to base lockdown policies on, but this has not prevented politicians from acting as if everything they say or do is based on solid science. The lockdown would not be merited if we were to genuinely adopt a knowledge-based approach. If we look at early projections by Neil Ferguson of Imperial College in the UK, he had grossly overstated the number of possible deaths resulting from the coronavirus and has now backtracked substantially. Ferguson has a chequered track record, which led UK newspaper The Telegraph to run a piece entitled ‘How accurate was the science that led to lockdown?’ The article outlines Ferguson’s previous flawed predictions about infectious diseases and a number of experts raise serious questions about the modelling that led to lockdown in the UK. Ferguson’s previous modelling for the spread of epidemics was so off the mark that it may beggar believe that anyone could have faith in anything he says, yet he remains part of the UK government’s scientific advisory group. Officials are now talking of ‘easing’ lockdowns, but Ferguson warns that lockdown in the UK will only be lifted once a vaccine for COVID-19 has been found. It raises the question: when will Ferguson be held to account for his current and previously flawed work and his exaggerated predictions? Because, on the basis of his modelling, the UK has been in lockdown for many weeks, the results of which are taking a toll on the livelihoods and well-being of the population which are and will continue to far outweigh the effects of COVID-19. According to a 1982 academic study, a 1% increase in the unemployment rate will be associated with 37,000 deaths [including 20,000 heart attacks, 920 suicides, 650 homicides], 4,000 state mental hospital admissions and 3,300 state prison admissions. Consider that by 30 April, in the US alone, 30 million had filed for unemployment benefit since the lockdown began. Between 23 and 30 April, some 3.8 million filed for unemployment benefit. Prior to the current crisis, the unemployment rate was 3.5%. Some predict it could eventually reach 30%. Ferguson – whose model was the basis for policies elsewhere in addition to the UK – is as much to blame as anyone for the current situation. And it is a situation that has been fuelled by a government and media promoted fear narrative that has had members of the public so afraid of the virus that many have been demanding further restrictions of their liberty by the state in order to ‘save’ them. Even with the promise of easing the lockdown, people seem to be fearful of venturing out in the near future thanks to the fear campaign they have been subjected to. Instead of encouraging more diverse, informed and objective opinions in the mainstream, we too often see money and power forcing the issue, not least in the form of Bill Gates who tells the world ‘normality’ may not return for another 18 months – until he and his close associates in the pharmaceuticals industry find a vaccine and we are all vaccinated. In the UK, the population is constantly subjected via their TV screens to clap for NHS workers, support the NHS and to stay home and save lives on the basis of questionable data and policies. Emotive stuff taking place under a ruling Conservative Party that has cut thousands of hospital beds, frozen staff pay, placed workers on zero-hour contracts and demonised junior doctors. It is also using the current crisis to accelerate the privatisation of state health care. In recent weeks, ministers have used special powers to bypass normal tendering and award a string of contracts to private companies and management consultants without open competition. But if cheap propaganda stunts do not secure the compliance, open threats will suffice. For instance, in the US, city mayors and local politicians have threatened to ‘hunt down’, monitor social media and jail those who break lockdown rules. Prominent conservative commentator Tucker Carlson asks who gave these people the authority to tear up the US constitution; what gives them the right to threaten voters while they themselves or their families have been exposed as having little regard for lockdown norms. As overhead drones bark out orders to residents, Carlson wonders how the US – almost overnight – transformed into a totalitarian state. With a compliant media failing to hold tyrannical officials to account, Carlson’s concerns mirror those of Lionel Shriver in the UK, writing in The Spectator, who declares that the supine capitulation of Britain to a de facto police state has been one of the most depressing spectacles he has ever witnessed. Under the pretext of tracking and tracing the spread of the virus, the UK government is rolling out an app which will let the likes of Apple and Google monitor a person’s every location visited and every physical contact. There seems to be little oversight in terms of privacy. The contact-tracing app has opted for a centralised model of data collection: all the contact-tracing data is not to be deleted but anonymized and kept under one roof in one central government database for ‘research purposes’. We may think back to Cambridge Analytica’s harvesting of Facebook data to appreciate the potential for data misuse. But privacy is the least concern for governments and the global tech giants in an age where ‘data’ has become monetized as a saleable commodity, with the UK data market the second biggest in the world and valued at over a billion pounds in 2018. Paranoia is usually the ever-present bedfellow of fear and many people have been very keen to inform the authorities that their neighbours may have been breaking social distancing rules. Moreover, although any such opinion poll cannot be taken at face value and could be regarded as part of the mainstream fear narrative itself, a recent survey suggests that only 20% of Britons are in favour of reopening restaurants, schools, pubs and stadiums. Is this to be the new ‘normal’, whereby fear, mistrust, division and suspicion are internalized throughout society? In an age of fear and paranoia, are we all to be ‘contact traced’ and regarded by others as a ‘risk’ until we prove ourselves by wearing face masks and by voluntarily subjecting ourselves to virus tests at the entrances to stores or in airports? And if we refuse or test positive, are we to be shamed, isolated and forced to comply by being ‘medicated’ (vaccinated and chipped)? Is this the type of world that’s soon to be regarded as ‘normal’? A world in which liberty and fundamental rights mean nothing. A world dominated by shaming and spurious notions of personal responsibility that are little more than ideological constructs of a hegemonic narrative which labels rational thinking people as ‘anti-science’ – a world in which the scourge of authoritarianism reigns supreme. * * * As this article was going to press, it was announced that Neil Ferguson is resigning from his role as science advisor to Boris Johnson’s government, in the wake of the allegations he has broken the lockdown rules he himself recommended in order to meet his girlfriend . |
|

After mounting evidence, FDA, CDC now admit that coronavirus tests are faultyWednesday, December 02, 2020 by: Franz Walker https://www.naturalnews.com/2020-12-02-coronavirus-tests-faulty-mounting-evidence.html (Natural News) For the past months, government agencies such as the Centers for Disease Control and Prevention (CDC) and the Food and Drug Administration (FDA) have been relying on Wuhan coronavirus (COVID-19) testing results to track the spread of the pandemic. But in recent months, both agencies have begun to concede that the testing methods that they’re using may not be as accurate as they would want them to be. They acknowledge that an increasing number of so-called positive test results are actually false positives. FDA acknowledges false-positives increase as actual cases go downOn Nov. 3, the FDA released new guidelines for rapid antigen testing for COVID-19 that acknowledged a high likelihood of incorrect results. The guidelines stated that health care professionals “should expect some [false-positive] results to occur.” These would occur even when “very accurate” tests were used to screen large populations with “a low prevalence of infection.” The FDA stated that the accuracy of rapid tests depends almost totally on the amount of COVID-19 in the population being tested, stating: “As disease prevalence decreases, the percent of test results that are false positives increase.” As an example, the FDA stated that a test with 98 percent specificity would accurately screen “just over 80% in a population with 10% prevalence.” This would mean that 20 out of 100 positive results would be false positives. The agency added that in a population with only a one percent prevalence, only 30 percent of those who test positive for the disease would actually have it. “Health care providers should take the local prevalence into consideration when interpreting diagnostic test results,” the FDA emphasized. The prevalence rate of COVID-19 has actually been quite low in a number of states. It has been recorded as between zero and 1.79 percent in Idaho and 6.4 percent in Pennsylvania. Meanwhile, the CDC estimated its prevalence in the New Orleans metropolitan area to be at around seven percent. The FDA also details a number of additional reasons for rapid testing inaccuracies. These included cross-contamination and complications in processing samples in batches. (Related: Coronavirus testing can be manipulated to make vaccines look more effective.) CDC agrees with FDA, also calls PCR tests into questionThe CDC has echoed the FDA’s recommendations. It stated that antigen tests “are not 100% accurate,” conceding that false positive and false negative results may occur. “Antibody test results should not be used to determine if someone can return to work,” the CDC stated, adding that this also applied to schools, dormitories and even correctional facilities. “People who receive positive results on an antibody test but don’t have symptoms of COVID-19 and have not been around someone who may have COVID-19 are not likely to have a current infection,” the agency explained, stating that these people can “continue with normal activities.” The CDC had already issued similar guidelines in August. That same month, a study published in the Journal of Clinical Microbiology found that rapid tests with a 98 percent specificity used in American schools could result in over 800,000 false-positive results every week. The CDC’s concerns over the accuracy of coronavirus testing extend beyond the rapid antigen test. In November, it highlighted a study that showed that screening for a single polymerase chain reaction (PCR) test only caught around 53 percent of all positive cases of COVID-19 in students returning home from college. The main protocol for PCR testing for COVID-19 has itself come into question after a study that claimed that PCR nasal swabs had a 63 percent sensitivity failed to provide a peer-reviewed report. At the end of November, an international group of scientists called for the paper’s retraction, calling it “severely flawed with respect to its biomolecular and methodological design.” Around the world, governments have already questioned the effectiveness of PCR testing. Portugal recently deemed the method unreliable. Meanwhile, other legal challenges to it are pending in Germany, Italy, Switzerland and South Africa. Follow Pandemic.news for more on the latest updates on the coronavirus pandemic. Sources include: |
|
Epidemiologist Says Influenza Cases Are Being Counted As COVID-19by Tyler Durden Top epidemiologist Knut Wittkowski says that the massive drop in influenza cases can be attributed to the fact that many are being falsely counted as COVID-19 cases.
 Person wearing Covid mask
Wittkowski, former Head of Biostatistics, Epidemiology and Research Design at Rockefeller University, cautioned that, “Influenza has been renamed COVID-19 in large part.” According to CDC figures, the cumulative positive influenza test rate from late September into the week of December 19th was just 0.2%, compared to 8.7% from a year before. According to Wittkowski, this is because many flu infections are being incorrectly labeled as coronavirus cases.
Those patients may “also may have some SARS RNA sitting in their nose while being infected with Influenza, in which case the influenza would be ‘confirmed’ to be COVID-19,” he added.
 Flu and Covid cases 2016 -2020
Wittkowski challenges the notion that masks and social distancing have resulted in a drop in flu cases, asserting that flu and COVID-19 viruses are “more similar than people want to acknowledge.”
In places like California and Pennsylvania where mask wearing is most common, COVID-19 cases have continued to skyrocket. As Just the News notes, “Data indicate that more than nine out of every 10 Americans in most states are wearing masks in public regularly; those numbers have been above 80% since the early fall. Yet average positive COVID-19 tests have multiplied by nearly seven times since the spring peak.” * * * New limited edition merch now available! Click here. In the age of mass Silicon Valley censorship It is crucial that we stay in touch. I need you to sign up for my free newsletter here. Support my sponsor – Turbo Force – a supercharged boost of clean energy without the comedown. Also, I urgently need your financial support here. |
|
States do battle with Biden administration over COVID lockdowns and mask mandatesThe more the Biden administration tightens its grip, the more states will slip through its fingers.Libby Emmons Brooklyn, NY 04March2021 8:29 PM https://thepostmillennial.com/states-do-battle-with-biden-administration-over-covid-lockdowns-and-mask-mandates Governors in several red states have spoken and have lifted their COVID restrictions on business and school closures, as well as the mask mandate that Biden requested be in effect at least for his first 100 days in office. Florida and South Dakota led the way in refusing to instigate lockdowns at all, but now Texas, Mississippi, and other states are following suit. The Biden administration isn’t happy about it. President Biden said those who were engaging in reopening were partaking in “Neanderthal thinking,” while White House Press Secretary Jen Psaki accused the governors of “ignoring the science.” Dr. Anthony Fauci said plainly “it just is inexplicable why you would want to pull back now, I understand the need to want to get back to normality but you’re only going to set yourself back if you just completely push aside the public health guidelines particularly when we’re dealing with 55-75,000 infections per day in the United States. That’s a very high baseline.”
 The-Post-Millennial-tweet-04March2021-Dr-Fauci WATCH: Dr. Fauci calls out states for reopening their economies, saying “it just is inexplicable why you would want to pull back now.”
But what Fauci and the entire Biden administration is missing are two key factors that make their positions on lockdowns and masking entirely irrelevant: the case, hospitalization, and death counts due to COVID in locked down states is comparable to those in non-locked down states. California and Florida are about the same, even though California is an incredibly young state while Florida’s population is more than 20 percent geriatric. If California, which has been extreme in their lockdown and masking rules, cannot manage to contain the virus, then there is no argument that lockdowns are effective. Additionally, these are American lives we’re talking about on both sides of the lockdown debate. On the one hand, Americans are getting sick and dying due to COVID. On the other, Americans are out of work, unable to care for their families, losing their homes, committing suicide, and being denied an education. If lockdowns don’t work, as they appear entirely not to, then keeping the economies of our states closed on the off chance that if we all comply that compliance will be effective is not a logical position. And people will not comply. We cannot press Americans into subservience to government fallacies any longer. Governor Ron DeSantis of Florida knows this plainly, and the atmosphere in his state is gloriously open and life-like. DeSantis said at CPAC: “Every Floridian has a right to earn a living,” citing the statistics on COVID cases, hospitalizations, and deaths. “Florida got it right and the lockdown states got it wrong.” Texas’ Governor Abbott said on March 2 that “Effective next Wednesday, all businesses of any type are allowed to open 100 percent,” Abbot proclaimed. “That includes any type of entity in Texas.” New York’s Governor Andrew Cuomo, who was given emergency powers by the state legislators that they are now trying to claw back, has given no real indication of when widespread reopening would be permitted to happen. Instead, he metes out allowable capacity percentages and floats plans for vaccine passports. California Governor Gavin Newsom, who presides over the state with some of the most rigid lockdowns and highest deaths, has called the Texas governor’s plans “absolutely reckless,” though his efforts have been no better. Due to the effects of the restrictions, they have been worse. Americans no longer have the time for these elitist leaders who don’t even follow their own mandates and restrictions, they no longer have the patience to watch their children, businesses, and families suffer under the weight of these orders. The more the Biden administration tightens its grip, the more states will slip through its fingers. The federal government should work with the governors, with the American people, to reopen the nation, not continue to demand adherence to mandates and orders that have proven to be ineffective. |
|
If Lockdowns Are Needed, Why Did More People Die In States That Locked Down Than Those That Didn’t?by Tyler Durden April 19, 2021 – https://www.zerohedge.com/covid-19/if-lockdowns-are-needed-why-did-more-people-die-states-locked-down-those-didnt One of the great things about America is that it has 50 states that can set their own policy across a broad range of areas, including on public health and lockdowns. This has allowed some to resist the stampede to impose swingeing restrictions on normal life in the hope of limiting transmission of SARS-CoV-2, and this provides us with a valuable control group in the great lockdown experiment that can give us an idea what might have happened if we hadn’t made some intervention or other. During the autumn and winter a new surge in Covid infections prompted most US states, like most Western countries, to reimpose restrictions. But a few resisted. Eleven states did not impose a stay-at-home order and left people at liberty to leave their homes whenever they wished. Of these, four – Florida, Georgia, South Carolina and South Dakota – did not impose any restrictions at all and treated it pretty much like any other winter. Although there are various differences between states that might have affected Covid outcomes, because they all form part of one country there are enough similarities to make comparisons useful. In particular, if lockdowns are effective and necessary to prevent hundreds of thousands of extra deaths (or the equivalent for the size of the population), then those states which didn’t lock down should have a far worse death toll. If the death tolls are not much worse, but about the same (or better), then lockdowns cannot be having a large impact on preventing Covid deaths. 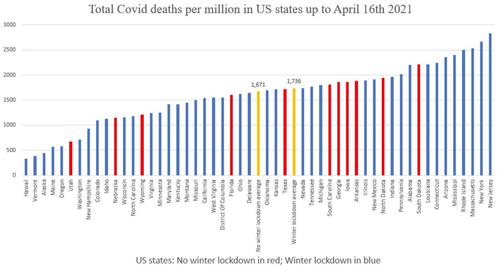 Total Covid-19 Deaths per million-by State-16April2021 In the chart above I have used data from Worldometer to plot the current total Covid deaths per million for each state. I have coloured the 11 states which did not lock down (i.e., impose a stay-at-home order) this winter in red. I have also calculated the average for the two groups of states, those which did not lock down over the winter and those which did, and coloured them in yellow. As you can see, states which did not lock down over the winter, far from having many times more Covid deaths, have actually had fewer – 1,671 vs 1,736 deaths per million. There may be demographic or other reasons that some states have a higher or lower number of deaths than others so we shouldn’t read too much into the precise differences. But even so, if lockdowns are supposed to suppress the virus to low levels and thus prevent ‘hundreds of thousands’ of deaths (or the population equivalent), then how is this possible? The only conclusion is that lockdowns do not work as intended and do not suppress the virus. This conclusion is reinforced by looking at the death tolls in the four states which imposed no restrictions at all over the winter, the average of which is 1,716 deaths per million, which is still below that of those which imposed lockdowns (1,736). Florida reopened in the autumn, Georgia and South Carolina in the spring of 2020, and South Dakota never closed. Yet overall they have suffered fewer Covid deaths per million than the states which imposed stay-at-home lockdowns this winter. Those academic teams which produce models predicting doom for places which don’t impose the measures they recommend should be challenged to apply their models to these states and hindcast the last winter. Any model which cannot accurately reproduce the known outcomes for these states should be calibrated until it can. Otherwise, if it can’t get the answer right for the past, why should we trust it for the future? The modelling teams at Warwick, Imperial and LSHTM can be found on Twitter (as can LSHTM’s Adam Kucharski) if anyone feels like putting these questions to them. |
|
Why The COVID-19 Model That Inspired UK’s Lockdown May Be “The Most Devastating Software Mistake Of All Time”by Tyler Durden 18May2020 – 02:45 https://www.zerohedge.com/geopolitical/why-covid-19-model-inspired-uks-lockdown-may-be-most-devastating-software-mistake-all-time While Democrats in the US and progressives in the UK continue to push back against efforts to gradually reopen their respective economies, more evidence is emerging that calls into question the models (what the public often refers to as the “science”) which inspired governments across the world to impose crippling lockdowns on their populations. Case in point: Since Neil Ferguson and the authors of the Imperial published its modeling for non-pharmaceutical intervention for COVID-19, a number of data scientists have taken a close look and found gaping oversights that seriously undermine the model’s credibility. Of course, this isn’t the first time we have written about Ferguson and his exploits. In this weekend’s Telegraph, two of these critics, David Richards, the founder and CEO of global big data leader WANdisco which is jointly headquartered in Silicon Valley and Sheffield, and Dr. Konstantin Boudnik, a pioneering big-data engineer, WANdisco’s VP of architecture and author of 17 US patents, published an editorial in which they carefully examined the model’s shortcomings. Keep in mind, the Imperial model is what ultimately inspired PM Boris Johnson to make a U-turn and adopt what has been an economically devastating lockdown – was nothing short of a catastrophe. Millions have been plunged into hardship and poverty unnecessarily, they explained. Johnson himself was infected by the virus and the public is furious with the government over its rollout of a plan to reopen. Given the influence the model had during the early days of the outbreak, the two men argued that the software issues underpinning the model could be ‘the most devastating software mistake of all time’. Apparently, the model’s problems are rooted in its most fundamental components. The model was written using a coding language called Fortran which has been in use for decades. Due to its age and inflexibility, Fortran has many inherent problems. But on top of the language itself, the code in the model was sprawling, sloppily written and extremely inefficient, the two men said, claiming it would never pass muster in the private sector. Using straightforward, jargon-free language, the two authors explain how the model ran into a problem called “CACE”, or, ‘changing anything changes everything’ – a problem that software engineers and data scientists trying to model, well, anything, really, often encounter.
It’s just the latest reminder that President Barack Obama’s advice to this year’s graduates rings true: You can’t just blindly accept what the experts and the people in charge tell you. Read the full editorial below: * * * In the history of expensive software mistakes, Mariner 1 was probably the most notorious. The unmanned spacecraft was destroyed seconds after launch from Cape Canaveral in 1962 when it veered dangerously off-course due to a line of dodgy code. But nobody died and the only hits were to Nasa’s budget and pride. Imperial College’s modelling of non-pharmaceutical interventions for Covid-19 which helped persuade the UK and other countries to bring in draconian lockdowns will supersede the failed Venus space probe and could go down in history as the most devastating software mistake of all time, in terms of economic costs and lives lost. Since publication of Imperial’s microsimulation model, those of us with a professional and personal interest in software development have studied the code on which policymakers based their fateful decision to mothball our multi-trillion pound economy and plunge millions of people into poverty and hardship. And we were profoundly disturbed at what we discovered. The model appears to be totally unreliable and you wouldn’t stake your life on it. First though, a few words on our credentials. I am David Richards, founder and chief executive of WANdisco, a global leader in Big Data software that is jointly headquartered in Silicon Valley and Sheffield. My co-author is Dr Konstantin ‘Cos’ Boudnik, vice-president of architecture at WANdisco, author of 17 US patents in distributed computing and a veteran developer of the Apache Hadoop framework that allows computers to solve problems using vast amounts of data. Imperial’s model appears to be based on a programming language called Fortran, which was old news 20 years ago and, guess what, was the code used for Mariner 1. This outdated language contains inherent problems with its grammar and the way it assigns values, which can give way to multiple design flaws and numerical inaccuracies. One file alone in the Imperial model contained 15,000 lines of code. Try unravelling that tangled, buggy mess, which looks more like a bowl of angel hair pasta than a finely tuned piece of programming. Industry best practice would have 500 separate files instead. In our commercial reality, we would fire anyone for developing code like this and any business that relied on it to produce software for sale would likely go bust. The approach ignores widely accepted computer science principles known as “separation of concerns”, which date back to the early 70s and are essential to the design and architecture of successful software systems. The principles guard against what developers call CACE: Changing Anything Changes Everything. Without this separation, it is impossible to carry out rigorous testing of individual parts to ensure full working order of the whole. Testing allows for guarantees. It is what you do on a conveyer belt in a car factory. Each and every component is tested for integrity in order to pass strict quality controls. Only then is the car deemed safe to go on the road. As a result, Imperial’s model is vulnerable to producing wildly different and conflicting outputs based on the same initial set of parameters. Run it on different computers and you would likely get different results. In other words, it is non-deterministic. As such, it is fundamentally unreliable. It screams the question as to why our Government did not get a second opinion before swallowing Imperial’s prescription. Ultimately, this is a computer science problem and where are the computer scientists in the room? Our leaders did not have the grounding in computer science to challenge the ideas and so were susceptible to the academics. I suspect the Government saw what was happening in Italy with its overwhelmed hospitals and panicked. It chose a blunt instrument instead of a scalpel and now there is going to be a huge strain on society. Defenders of the Imperial model argue that because the problem – a global pandemic – is dynamic, then the solution should share the same stochastic, non-deterministic quality. We disagree. Models must be capable of passing the basic scientific test of producing the same results given the same initial set of parameters. Otherwise, there is simply no way of knowing whether they will be reliable. Indeed, many global industries successfully use deterministic models that factor in randomness. No surgeon would put a pacemaker into a cardiac patient knowing it was based on an arguably unpredictable approach for fear of jeopardising the Hippocratic oath. Why on earth would the Government place its trust in the same when the entire wellbeing of our nation is at stake? * * * Source: The Telegraph |
|
Professor Explains Flaw In Many Models Used For COVID-19 Lockdown Policiesby Tyler Durden 11May2021 – https://www.zerohedge.com/political/professor-explains-flaw-many-models-used-covid-19-lockdown-policies Authored by Andrew Chen via The Epoch Times (emphasis ours), Economics professor Doug Allen wanted to know why so many early models used to create COVID-19 lockdown policies turned out to be highly incorrect. What he found was that a great majority were based on false assumptions and “tended to over-estimate the benefits and under-estimate the costs.” He found it troubling that policies such as total lockdowns were based on those models.
Allen says most of the early cost-benefit studies that he reviewed didn’t try to distinguish between mandated and voluntary changes in people’s behaviour in the face of a pandemic. Rather, they just assumed an exponential growth of cases of infection day after day until herd immunity is reached. In a paper he published in April, in which he compiled his findings based on a review of over 80 papers on the effects of lockdowns around the world, Allen concluded that lockdowns may be one of “the greatest peacetime policy failures in Canada’s history.” He says many of the studies early in the pandemic assumed that human behaviour changes only as a result of state-mandated intervention, such as the closing of schools and non-essential businesses, mask and social distancing orders, and restrictions on private social gatherings. However, they didn’t take into consideration people’s voluntary behavioural changes in response to the virus threat, which have a major impact on evaluating the merits of a lockdown policy. “Human beings make choices, and we respond to the environment that we’re in, [but] these early models did not take this into account,” Allen said. “If there’s a virus around, I don’t go to stores often. If I go to a store, I go to a store that doesn’t have me meeting so many people. If I do meet people, I tend to still stand my distance from them. You don’t need lockdowns to induce people to behave that way.” Allen’s own cost-benefit analysis is based on the calculation of “life-years saved,” which determines “how many years of lost life will have been caused by the various harms of lockdowns versus how many years of lost life were saved by lockdowns.” Based on his lost-life calculation, lockdown measures have caused 282 times more harm than benefit to Canadian society over the long term, or 282 times more life years lost than saved. Furthermore, “The limited effectiveness of lockdowns explains why, after one year, the unconditional cumulative deaths per million, and the pattern of daily deaths per million, is not negatively correlated with the stringency of lockdown across countries,” writes Allen. In other words, in his assessment, heavy lockdowns do not meaningfully reduce the number of deaths in the areas where they are implemented, when compared to areas where lockdowns were not implemented or as stringent. Today, some 14 months into the pandemic, many jurisdictions across Canada are still following the same policy trajectory outlined at the beginning of the pandemic. Allen attributes this to politics. He says that politicians often take credit for having achieved a reduction in case numbers through their lockdown measures. “I think it makes perfect sense why they do exactly what they did last year,” Allen said. “If you were a politician, would you say, ‘We’re not going to lock down because it doesn’t make a difference, and we actually did the equivalent of killing 600,000 people this last year.’” You wouldn’t, he said, because “the alternative is they [politicians] have to admit that they made a mistake, and they caused … multiple more loss of life years than they saved.” Allen laments that media for the most part have carried only one side of the debate on COVID-19 restrictions and haven’t examined the other side. Adding to the concern, he says, is that views contrary to the official government response are often pulled from social media platforms. He says he has heard that even his own published study has been censored by some social media sites. “In some sense these are private platforms. They can do what they want. But on the other hand, I feel kind of sad that we live in the kind of a world where posing opposing opinions is either dismissed, ignored, or … name-called, [and] in some ways cancelled,” Allen said. |
|
“Tourist Go Home” – Tensions Soar As Hawaiians Urge Non-Residents To “Leave”by Tyler Durden 20April202020 https://www.zerohedge.com/health/tourist-go-home-tensions-soar-hawaiians-urge-non-residents-leave
Nefesh B’Nefesh: Live the Dream US & CAN 1-866-4-ALIYAH | UK 020-8150-6690 or 0800-085-2105 | Israel 02-659-5800 https://www.nbn.org.il/ info@nbn.org.il Hawaiians are becoming increasingly angry, not because the tourism industry has collapsed, and 37% of the labor force has just filed for unemployment, but mostly because US mainlanders, motivated by super discounted flights and hotel rooms, continue to pour into the various Hawaiian Islands during the pandemic. Troy Kane, a local on Oahu, who was interviewed by The Guardian, said residents are abiding by the stay-at-home orders as cases and deaths surge. He points out tourists on the island are ignoring social distancing rules and risk spreading the virus to locals.
The Guardian says, “$100 airfares” are enticing people in quarantine in the continental US to vacation in Hawaii. Last week, nearly 800 tourists arrived on the islands. The influx triggered a nerve among locals and officials who argue tourists need to leave. As of Monday, 580 cases and ten deaths have been confirmed across the Hawaiian Islands. About 35 cases have been non-residents. 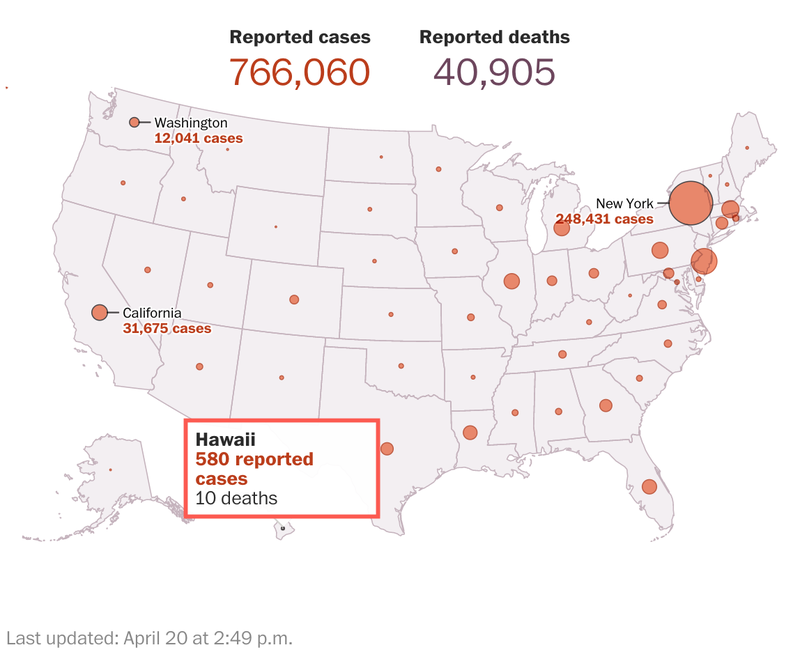 US Coronavirus Map 20April2020 Kane is a neighborhood board member and community representative of Waimanalo and says the native Hawaiian and Micronesian populations on the islands are at higher risk of contracting the disease. He worries for his community and family that tourists are blatantly disregarding the public health order. “People will always see this place as their playground. And in this moment, as a Native Hawaiian, this is very reflective of many historical circumstances, where people from outside of the islands have come in and caused real harm to the native population. It’s not always with the direct intent to do so, but the impacts, especially on Hawaiian people, are very real,” he said.
Hawaiians last month protested tourists arriving at the Maui airport. Some held signs that said: “TOURIST GO HOME,” “LEAVE OUR AINA!,” “TIME TO GO,” and “GO HOME.”  Maui residents protesting tourist near airport on 21March2020. h/t Star-Advertiser
 Protester near airport on 21March2020. h/t Star-Advertiser
 Protesters near Maui airport on 21March2020 h/t Star-Advertiser Josh Masslon, a Maui-based ICU nurse, said the healthcare system on the islands does not have enough capacity to handle a virus outbreak.
Masslon said he’s called the police on tourists for breaking the public health order. So, at what point do Hawaiians, fed up with ignorant tourists breaking social distancing rules and risk infecting the local community, take the law into their own hands and start blocking airport exits, preventing new arrivals from entering?
Hawaii Arrests ‘Rogue Tourists’ In COVID Contagion Crackdownby Tyler Durden 08May2020 – https://www.zerohedge.com/health/hawaii-arrests-rogue-tourists-covid-contagion-crackdown As the travel and tourism industry implodes, savvy consumers, with zero f*cks given about contracting the virus, have been buying cheap airfare to Hawaii, along with heavily discounted rooms at top resorts. Around mid/late March, when strict stay-at-home orders went into effect, locals, who were confined to their homes, noticed many of these tourists were disregarding public health orders. This infuriated some who allege that if an outbreak on the island(s) was seen, it could easily overwhelm the local hospital system. By late March, tensions between locals and tourists were quickly building. A group of locals held a protest at Kahului Airport in Maui County, holding up signs that read: “TOURIST GO HOME,” “LEAVE OUR AINA!,” “TIME TO GO,” and “GO HOME.”
By mid-April, the Hawaii Tourism Authority issued a $25,000 grant to nonprofit Visitor Aloha Society of Hawaii (VASH) to fund a program that would issue one-way plane tickets to tourists who broke 14-day quarantine orders or other social distancing rules. As of April 26, we noted about 26 tourists were provided one-way tickets back to their home airports for breaking the rules. Now it appears things are getting serious in the state. Authorities are arresting “rogue tourist” who break quarantine orders:
The strict measures, some of the most stringent in the country, have been working to suppress the outbreak. As of Friday, about 629 cases and 17 deaths have been reported in the state, a relatively low number when compared with Northeast states.
Hawaii sacrificed its largest industry: tourism – to fend off the virus. With many resorts, restaurants, and other businesses closed, unemployment has skyrocketed to 25% to 35%. At least 100 hotels have suspended operations as locals stay home to weather the public health crisis.
Honolulu City Councilmember Kym Pine said the sacrifices Hawaiians are making today to protect their communities, in the long run, is hugely disrespectful when a tourist comes to the state and blatantly ignores the rules.
AP says the honeymooning couple, Borice Lepovskiy, 20, and Yuliia Andreichenko, 26, of California, refused to sign a “quarantine agreement” after they came back late one night after picking up pizza. The next morning, they left their room and were arrested. At least 20 people have been arrested statewide on charges of breaking quarantine orders. Many others have been given warnings or citations. Anyone who is convicted of the violation is subjected to a $5,000 fine and a year in jail. “Officials have even considered having travelers wear an ankle bracelet during their quarantine period, or setting up a designated site where tourists would be required to stay at for the 14 days,” AP notes. Mufi Hannemann, president and CEO of Hawaii Lodging and Tourism Association, said hotel key cards are being programmed to only allow people to check-in – so when they leave their rooms – they will need to get a new card, which would be a red flag for front-desk workers that the tourist potentially violated quarantine rules. AP provides several other accounts of tourists being arrested:
And a word to the wise – it’s probably a good idea to stay away from Hawaii at the moment. The next thing you know, law enforcement might start tracking tourists with GPS bracelets. |
|
Some Bad News From JPMorgan:This Is What Happens After We Pass The Virus Peakby Tyler Durden 07April2020 https://www.zerohedge.com/health/some-bad-news-jpm-what-happens-after-we-pass-virus-peak Yesterday, when giving an update on the global coronavirus infection curve, and highlighting where various nations currently reside on the curve, we said what has become conventional wisdom, namely that “with every passing day, the world – most of which is currently on lock down – gets closer to the infection inflection point, and as the updated “corona curve” chart shows, all the nations that were in the exponential rise phase (acceleration), are now moving into the stage of infection growth rate slowdown (accumulation), suggesting that a peak for most countries is now just a matter of time, at which point the number of new cases will start slowing down aggressively. This means that while US cases continue to soar, the light at the end of the tunnel is now visible.” 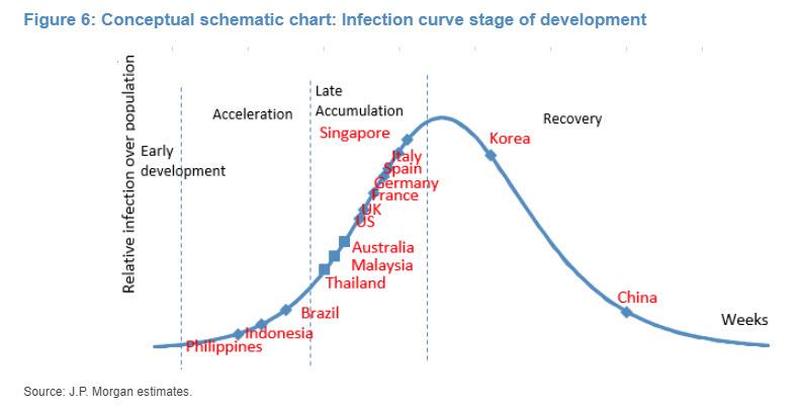 infection growth rate curve stage Some, such as JPMorgan’s delightfully permabullish quant Marko Kolanovic (who is so keen on giving flashbacks to his notes from x weeks ago, if not so much his “once in a decade” call to buy value/short low-vol stocks last July), ran with this data to its extreme conclusion, writing today that his models “have indicated that social distancing is working and that the apex of the pandemic will come sooner and require significantly less peak hospitalizations than projected by the models used by government officials at the time.” In short, it’s all downhill from here on the corona-curve… literally, which is great news if that was all there is to it as every analyst-trader-amateur-epidemiologist jumps to conclude. Unfortunately, it turns out that there is much more to it what happens next than “conventional wisdom” hot takes and amateur Wall Street virologists would have you believe, because in a separate not from a far more erudite JPM analyst – at least when it comes to coronavirus analysis – the bank’s MW Kim writes that the first apex is just the beginning, and then – as China is learning now as it reports the most new cases in a month… 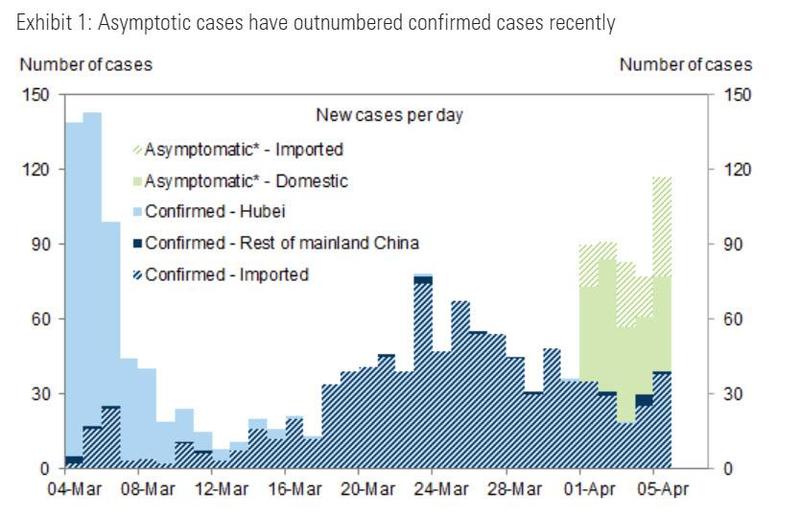 Asymptotic cases vs confirmed cases … it gets much worse again as the second infection wave is unleashed, then the third, and so on. So what’s really going on? First let’s do the good news, which as JPM’s MW Kim notes, have to do with the slowdown in global infections which grew 62% w/w to 1,275,542, while infection growth momentum has slowed compared to ~95% w/w ten days ago. 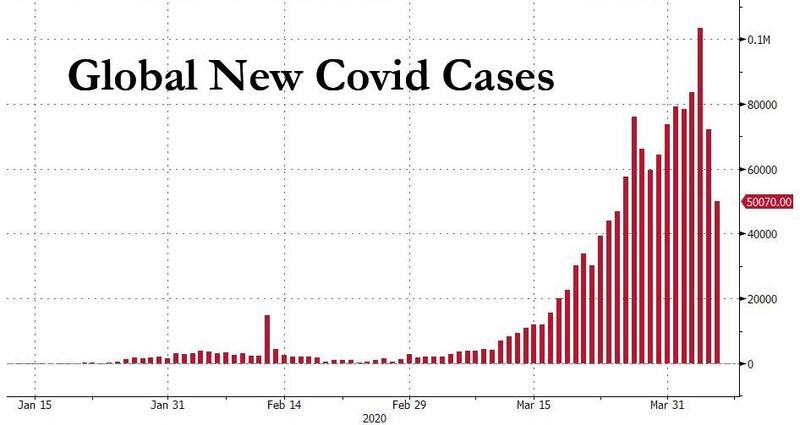 Global new Covid-19 Cases 07April2020 Furthermore, as we reported yesterday, several of the larger impacted countries are now in the slower infection growth rate accumulating stage (the latest curve chart as of this morning is shown below)… 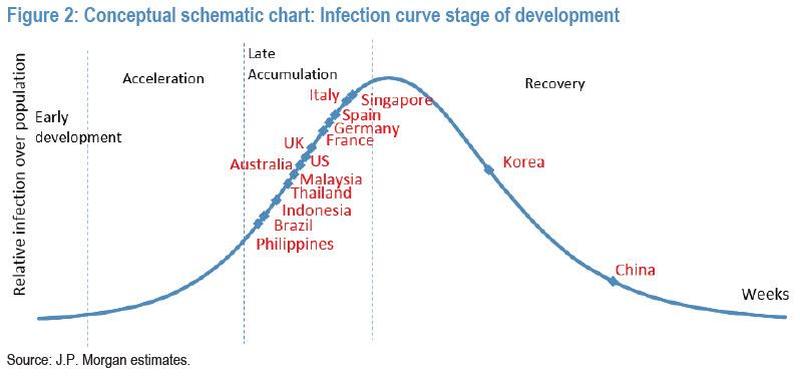 infection growth rate curve stage 07April2020 … and JPM is optimistic that post Easter holidays, market focus could likely shift towards “infection peak”/ “recovery statistics” from the current ‘daily new additions’. Now, and as is customary, are the not so good news: MW Kim cautions that his findings on COVID-19 so far include (1) the lack of a vaccine makes it difficult to clear the virus; (2) social distancing is an expensive strategy in terms of economic/ social cost perspective; (3) it may perhaps prove challenging to build popular acceptance of stricter social distancing for more than a month. Therefore, and this is the key part, JPMorgan (at least the non-quant part of JPMorgan) “cannot rule out the possibility that global infection curves propagate secondary waves, shaped similar to seismic aftershocks until a vaccine is broadly available.” Some more details from JPM on how and why “reducing new contacts” aka social distancing has been the primary containment strategy:
So far so good, and social distancing does indeed show success. But, as JPM asks, the question is if authorities will face challenges in acceptance to extend strict social-distancing for longer periods (say over a month). Therefore, the bank’s analyst cannot rule out the possibility that successive global infection curves form until a vaccine is broadly available. The strategy then may shift to society living with COVID-19, but minimizing infection scale/scope. Which then brings us to the $64 trillion (roughly in line with global GDP) question: is the coming “second reinfection wave” going to be smaller or bigger, similar to the Spanish Flu pandemic, where deaths in the second wave were 5x greater than those from the first? 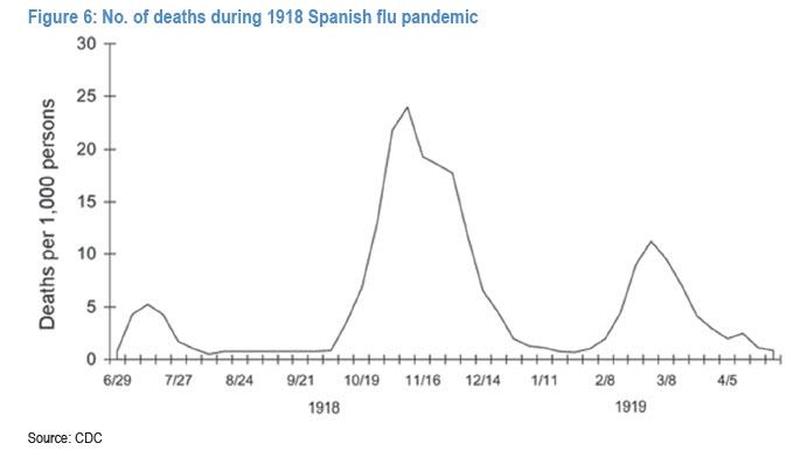 Deaths during 1918 Spanish flu Pandemic Here JPM believes that next waves could be at a smaller amplitude with lower mortality rate potential compared to the current first wave. This is due to (1) strong risk awareness among stakeholders; (2) faster government response potential at the infection tipping point; and (3) enhanced risk manual at the containment stage. However, even a substantially reduced amplitude of wave 2 (and 3 and 4), suggest that ongoing economic shutdowns will be recurring feature of life for quarters if not years!
 Coronavirus-global infection rate The amplitude could be higher, however, a la the Spanish Flu pandemic, if it turns out that the life cycle of the coronavirus is far longer than assumed. As JPM notes, the COVID-19 infection life cycle could last for 4-5 weeks including a 2-week incubation period. The bottom line, and somewhat counterintuitively, the sooner the world declares victory against the Wu Flu, the faster the general population will rush back into “social undistancing”, sparking countless new case clusters as the infection restarts from scratch, forcing authorities to re-establish social distancing once again, and so on, as the entire process repeats from square one. |
|

How Long Will the American Covid-19 Lockdown Last? Here’s What the Patterns SuggestMarch 29, 2020 by Daisy Luther https://www.theorganicprepper.com/how-long-covid-19-patterns/ (March 29, 2020) From the moment lockdowns and serious social distancing efforts began in the United States, the question on everyone’s mind was, “How long will these lockdowns last?” And it’s not simple impatience. The cost of Covid-19 continues to come as a brutal assault to families across the country. First, there was the money spent preparing for the likelihood of quarantine, and this was followed, for many, by a loss of income. A shocking 3.3 million people had filed for unemployment by last Thursday, something projected less than a week ago and laughed off by many as fear-mongering. The economic ramifications of this virus are not just short-term – they’re long-term too. It’s psychological, too. Right now, we’re in this strange period of purgatory in which the situation isn’t that bad for a lot of people – outside of a few hotspots, we aren’t seeing the virus in our own backyards. But the inability to plan for something next summer, next month – even next week – is tough on people who are accustomed to being able to map out things like vacations, summer activities for the kids, heck, even a night at the movies with our partners. There’s a sense of overall discomfort which can only be described as grief as we miss out on goals, milestones, and the day to day lives we enjoyed just a couple of short weeks ago. We want this to end. Now. And if we can’t have that, we want to know when. When will this limbo known as lockdown be over? Unfortunately, we’re just getting started.A few weeks ago, I wrote about when the lockdowns and shelter in place orders would be handed down in the United States, based on the patterns we were seeing in China and in Italy. It turned out to be extremely accurate, so we can use the same general idea of using patterns to attempt to predict what happens next. Now, keep in mind, there are all sorts of variables. I hate making “predictions because of this. These aren’t “predictions” in a crystal ball kind of way. This is just an analysis of what has already happened and how a pattern is developing. So, my disclaimer is, given the vast array of variables, some of which we’ve probably never even considered, these dates may be entirely wrong. But right now, patterns are all we have to give us an idea of what to expect. Some of the variables that could come into play are the severity of the lockdown, the population density of the infection hotspots, a surge of civil unrest, a concurrent disaster, and/or the medical systems in the different countries involved. China is a lot more authoritarian than the US and Italy, and they incorporated shocking measures like literally welding people into their apartments. While things started off rather gently in Italy and the United States, don’t expect it to stay that way. Italy started off less strictly but has increasingly become tougher on citizens as the cases explode, and we’re seeing harsher measures being instituted across the United States as governors take steps to protect their less-infected states from those fleeing hotspots. Expect this to continue up to and including martial law if people don’t cooperate with social distancing measures. I’m not saying that this is a good thing or a bad thing – I’m just pointing out that this is reality. If you don’t believe it, read this article about how the cops in Rhode Island are teaming up with the National Guard to go door to door looking for New Yorkers who have fled the city. Right here in the United States of America, boys and girls. Don’t delude yourself into thinking we’re protected by the Constitution right now. While that should always be the case, know that right now, we’re not. Some definitionsFor the purposes of this article, here are some definitions that I’m using.
The charts below are all from Worldometer and show the new cases diagnosed in each country. I’m not a scientist, a statistician, or a doctor. These are my definitions that I’ll be using throughout the article and I’m sharing them for the purpose of clarity so that we’re all reading from the same songbook. Here’s how it went down in China.Keep in mind that I never trusted and still do not trust the numbers coming from China. I’m not basing any of this on their numbers, but on their increases and decreases. If it helps any, I don’t trust the American numbers either. I’m equal opportunity in my distrust. All we’re looking at here are patterns. The lockdown of China began on Jan. 22. Within a few days, the lockdown had spread to incorporate millions and millions of people and were quite widespread to some degree or another. This is Worldometer’s chart for China. The chart begins on Jan. 22, which is not accurate – that was the day that they locked down Wuhan so we know there were a number of cases before that date. But this is the data we have to work with. Again, we’re not focused on the numbers, but on the pattern.
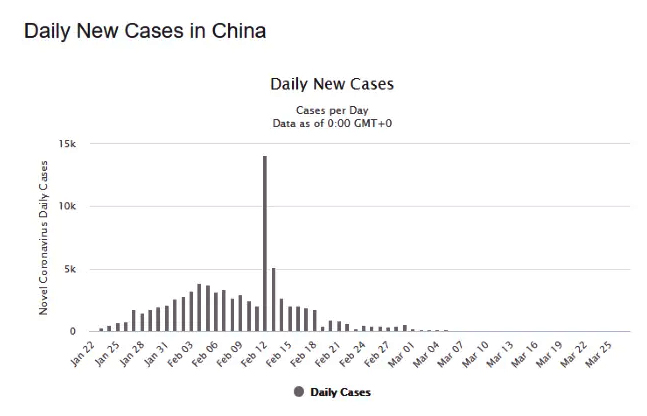 Worldometer’s chart for China China’s cases hit the plateau that we’re calling a “peak” approximately Jan. 30th. That’s when they hit a plateau that was continued after the peak until cases began to drop off on Feb. 19th. During this time, the cases were being diagnosed hard and fast at a high rate that varied from day to day but stayed in a certain range. This means the peak for China began 8 days after widespread lockdown and lasted for 20 days. You can see a spike on Feb. 13th and 14th. This can be explained away – at least in part. China began using a different diagnostic method on the 13th that didn’t require the antigen test. It was faster and easier to diagnose patients at that time. There were 15 thousand new cases that day and this is notable. This spike occurred 22 days after the lockdown began. They only used this diagnostic method for 2 days, then returned to their previous methods of diagnosis. At that time, numbers returned generally to the plateau that we’re calling the peak. Cases began to decline 21 days after the peak began, on Feb. 19th. 65 days after the lockdown began, Wuhan relaxed to the lockdown: people can leave their homes but are not allowed to leave the city. If all goes well, China plans to reopen Wuhan on April 8th which is 77 days after they first locked down Wuhan. We’ll learn a lot about our own future when we see how it goes in Wuhan a couple of weeks from now. Here’s the deal with Italy.Italy began its regional lockdown on Feb. 21st and it quickly expanded to a widespread national lockdown by March 9th. (source for dates) As I write this, Italy is at day 20 of its lockdown In the chart below, it appears that Italy began its peak around March 18th, which is 9 days after widespread lockdowns began.
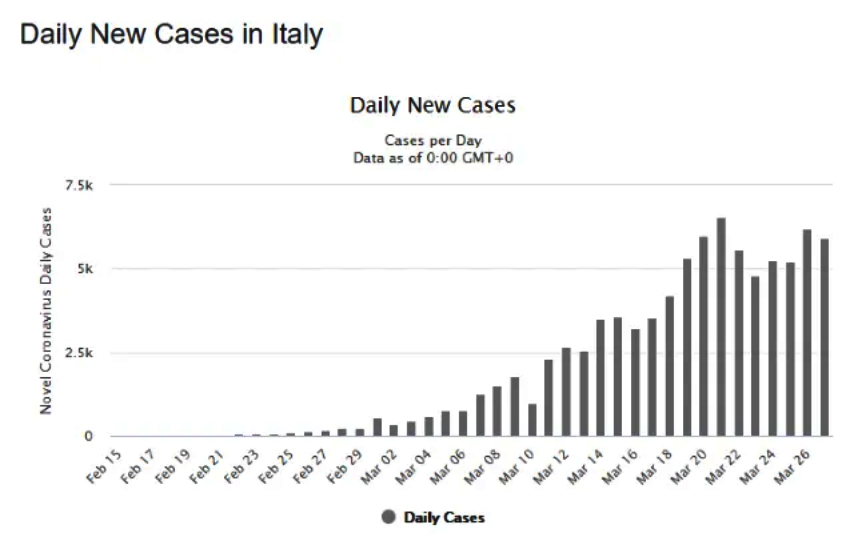 Worldometer’s chart for Italy If the same pattern as China holds true, infections will decline but still be in peak until April 20th. Italy could begin to relax its lockdown as of May 13th. If China does indeed completely lift its lockdown on Day 77 and this works well, then the end of Italy’s lockdown could be June 6th. Again, there are many variables. For example, on March 28th in Italy (yesterday at the time of writing), tensions arose in Italy as the health emergency became a social emergency. People broke the shelter in place orders, threatening to storm supermarkets because they’ve run out of food. Cries for revolution arose throughout social media and many people have said they will not remain at home, and that they’re out of food and basic necessities. This could, unfortunately, result in a much longer period of infection as people gather in crowds to protest. It could even result in a spike for Italy around March 31-April 1 that would be similar to China’s spike, albeit for a different reason. What about the US?First things first – this is not going to be over in two weeks. If the country reopened again next week or the week after while cases are still climbing, everything we’ve done from this point on will have been in vain. We’re in this social distancing business for quite a while if we want it to work. Our first major lockdowns began on March 19th. Thirty-three states have closed down non-essential businesses or mandated some type of lockdown since that time. If we base our timing on the pattern of China, the peak would have begun yesterday, March 28th. We should begin to see the curve flattening out on charts within the next few days.
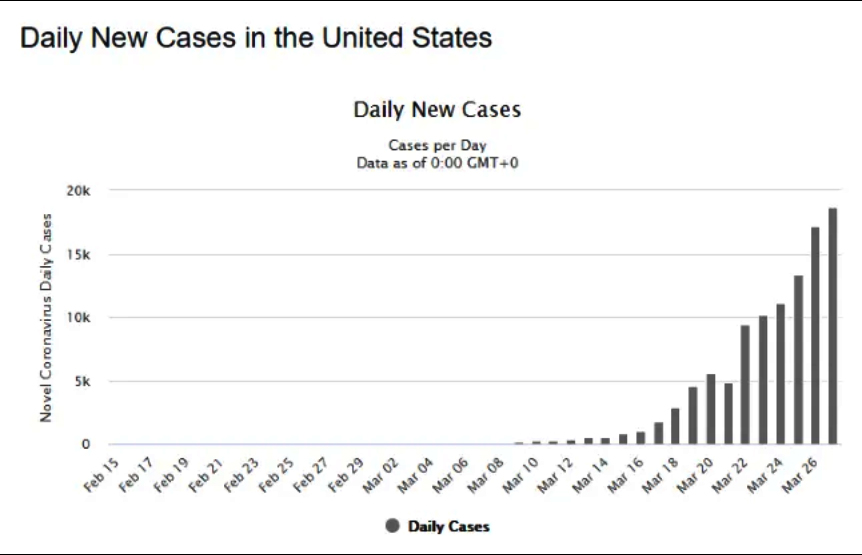 Worldometer’s chart for US This peak would last through about April 30th and we could see our worst days on April 10th and 11th, depending on whether we have some kind of unusual variables like both China and Italy have had. On May 23rd, we could see the lockdowns become more relaxed, and if they go 77 days like Wuhan, then the lockdowns would end on June 6th. It’s important to note that we still don’t know what the aftermath of the lockdown looks like in China. It could end up that they’ll put another lockdown in place if infections begin to reoccur at a high rate. Personally, I don’t plan to rush out to a crowded mall the moment lockdowns are lifted. I want to wait and see what happens after a week or so first. To provide an example, several hundred movie theaters in China outside the epicenter of the outbreak reopened on March 23rd, then were abruptly ordered to close on March 27th without further explanation. The reopening of the United States could also be a start-and-stop process as scientists learn more about Covid-19. This isn’t a short term event. It’s going to get worse.I’m not the only person who thinks these measures could last for quite some time. According to Michael Snyder, it will be ongoing and we too could expect to see some civil unrest before this is over.
As in China, there are parts of the country that are far less affected than places like New York City and New Orleans. But every single state has diagnosed Covid within its boundaries and none of the country is unscathed by the measures being undertaken to combat the spread. And despite the steps that Americans have taken to slow this down, we have the unfortunate distinction of surpassing China as the epicenter of the pandemic. On Thursday, March 26th, 17,224 new cases were diagnosed here and on Friday, there were 19,452 new cases. Unfortunately, the number of new cases is still climbing. We have not seen the worst of this situation yet. People should be prepared for anything from more stringent lockdowns, supply chain interruptions, and potentially even civil unrest in some areas as the situation drags on. I know these dates and numbers are probably not what you want to hear. It’s only been ten days and for many, it’s practically unimaginable to live like this for 2 more months, stretching into June. The effect on the economy alone is mindblowing, not to mention the feelings of uncertainty, unrest, and even fear that many people are experiencing. But if you’re anything like me, you’d rather go into this unknown territory facing reality instead of waiting and wondering. About DaisyDaisy Luther writes about current events, preparedness, frugality, voluntaryism, and the pursuit of liberty on her website, The Organic Prepper. She is widely republished across alternative media and she curates all the most important news links on her aggregate site, PreppersDailyNews.com. Daisy is the best-selling author of 4 books and runs a small digital publishing company. You can find her on Facebook, Pinterest, and Twitter. |
|
Just like in China Thousands Of COVID-19 Deaths Have Gone Uncounted In The USShocking Expose Proves Thousands Of COVID-19 Deaths Have Gone Uncounted In The US: Live Updatesby Tyler Durden 05April2020 https://www.zerohedge.com/geopolitical/new-york-reports-promising-first-drop-covid-19-deaths-hell-week-begins-live-updates * * *  Bodies are buried in a trench on Hart Island, Wednesday, April 8, 2020, in the Bronx borough of New York. (AP Photo/John Minchillo) Update (1445ET): Two reporters from the New York Times purport to have found evidence that health officials, often at the local or county level, are dramatically undercounting coronavirus deaths in the US. Citing information and documents provided by “doctors, hospital officials, public health experts and medical examiners,” among others, the reporters claim that potentially thousands of deaths have gone uncounted, meaning the total is probably closer to 20k – or beyond – than the roughly 10k (9,180, per JHU) reported so far. Unfortunately, since the patients have died, there will be few – if any – opportunities for these discrepancies to be rectified, if coronavirus isn’t listed as a cause of death, something that requires a positive test. Given the shortage of tests around the US, living patients have typically been prioritized over the deceased, even as counting posthumous deaths is important in helping officials get the accurate data they need to fight the virus. A lot of the most compelling anecdotes in the report came from coroners, and from families like this one, per the NYT:
Even Johns Hopkins University agreed that deaths are almost certainly being undercounted: “We definitely think there are deaths that we have not accounted for,” said Jennifer Nuzzo, a senior scholar at the Johns Hopkins University Center for Health Security. JHU has been tracking the virus from the beginning, maintaining an online database that has become one of the most trusted and widely-cited sources of data on deaths and cases by the press around the world. * * * |
|
Supplies Are Starting To Get Really Tight Nationwide As Food Distribution Systems Break Downby Tyler Durden 31March2020 https://www.zerohedge.com/health/supplies-are-starting-get-really-tight-nationwide-food-distribution-systems-break-down Authored by Michael Snyder via The End of The American Dream blog, All across America, store shelves are emptying and people are becoming increasingly frustrated because they can’t get their hands on needed supplies. Most Americans are blaming “hoarders” for the current mess, but it is actually much more complicated than that. Normally, Americans get a lot of their food from restaurants. In fact, during normal times 36 percent of all Americans eat at a fast food restaurant on any given day. But now that approximately 75 percent of the U.S. is under some sort of a “shelter-in-place” order and most of our restaurants have shut down, things have completely changed. Suddenly our grocery stores are being flooded with unexpected traffic, and many people are buying far more than usual in anticipation of a long pandemic. Unfortunately, our food distribution systems were not designed to handle this sort of a surge, and things are really starting to get crazy out there.
I would like to share with you an excerpt from an email that I was sent recently. It describes the chaos that grocery stores in Utah and Idaho have been experiencing…
With most of the country locked down, normal economic activity has come to a standstill, and it is going to become increasingly difficult for our warehouses to meet the demand that grocery stores are putting on them. Meanwhile, our farmers are facing severe problems of their own. The following comes from CNBC…
The chaos in the financial markets is likely to continue for the foreseeable future, and it is going to remain difficult for farm laborers to move around as long as “shelter-in-place” orders remain in effect on the state level. Iowa farmer Robb Ewoldt told reporter Emma Newburger that “we’ve stopped saying it can’t get worse”, and he says that this coronavirus pandemic looks like it could be “the straw that broke the camel’s back”…
Of course this comes at a time when millions of Americans are losing their jobs and unemployment is shooting up to unthinkable levels. Without any money coming in, many people are already turning to alternative sources of help in order to feed themselves and their families. On Monday, hundreds of cars were lined up to get food from a food bank in Duquesne, Pennsylvania. To many, this was eerily reminiscent of the “bread lines” during the Great Depression of the 1930s.
 Andrew Rush tweet 30March2020 Hundreds of cars wait to receive food from the Greater Community Food Bank in Duquesne. Collection begins at noon. @PghFoodBank @PittsburghPG
And it is also being reported that the number of people coming for free meals on Skid Row in Los Angeles has tripled since that city was locked down. Sadly, these examples are likely only the tip of the iceberg of what we will see in the months ahead. And it won’t just be the U.S. that is hurting. The following comes from a Guardian article entitled “Coronavirus measures could cause global food shortage, UN warns”…
If this pandemic stretches on for an extended period of time, food supplies are inevitably going to get even tighter. So what can you do? Well, perhaps you can start a garden this year if you don’t normally grow one. Apparently this pandemic has sparked a tremendous amount of interest in gardening programs around the country…
Food is only going to get more expensive from here on out, and growing your own food is a way to become more independent of the system. But if you don’t have any seeds right now, you may want to hurry, because consumer demand is spiking…
For years, I have been warning people to get prepared for “the perfect storm” that was coming, but of course most people didn’t listen. But now it is upon us. Desperate people have been running out to the grocery stores to stock up on toilet paper only to find that they are limited to one or two packages if it is even available. And now that “panic buying” of seeds has begun, it is probably only a matter of time before many stores start running out. We have reached a major turning point in our history, and things are only going to get crazier. Unfortunately, the vast majority of Americans still have absolutely no idea what is ahead of us… |
|
Grocers Begin to Stockpile and Build ‘Pandemic Pallets’ To Prepare For Winter Surge of COVID CasesSep 27, 2020 https://endtimeheadlines.org/2020/09/grocers-begin-to-stockpile-and-build-pandemic-pallets-to-prepare-for-winter-surge-of-covid-cases/ (ETH) – Grocery stores and food companies are reportedly preparing for what could be a coming increase in sales amid a new rise in Covid-19 cases and the coming Holidays.
According to the Wallstreet Journal, Supermarkets have already begun stockpiling groceries and storing them early to prepare for the coming fall and winter months, when some health experts are now warning the country could possibly face another widespread outbreak of coronavirus cases and new restrictions.
According to MSN News, Amid a surge in the Midwest, Minnesota has surpassed 2,000 deaths as Wisconsin and South Dakota reached a record number of cases and North Dakota just posted its second-highest number of cases as hospitals warned they were filling up. A new report from Reuters is stating that the number of tests returning positive for COVID-19 is topping 25% in several states across the U.S. Midwest as cases and hospitalizations also surge in the region. |
|
Hospitals consider universal do-not-resuscitate orders for coronavirus patientsWorry that ‘all hands’ responses may expose doctors and nurses to infection prompts debate about prioritizing the survival of the many over the oneBy Ariana Eunjung Cha 26March2020 https://www.washingtonpost.com/health/2020/03/25/coronavirus-patients-do-not-resucitate/ JerusalemCats Comments: This is Disaster or Battlefield Triage
Hospitals on the front lines of the pandemic are engaged in a heated private debate over a calculation few have encountered in their lifetimes — how to weigh the “save at all costs” approach to resuscitating a dying patient against the real danger of exposing doctors and nurses to the contagion of coronavirus. The conversations are driven by the realization that the risk to staff amid dwindling stores of protective equipment — such as masks, gowns and gloves — may be too great to justify the conventional response when a patient “codes,” and their heart or breathing stops. Northwestern Memorial Hospital in Chicago has been discussing a do-not-resuscitate policy for infected patients, regardless of the wishes of the patient or their family members — a wrenching decision to prioritize the lives of the many over the one. Richard Wunderink, one of Northwestern’s intensive-care medical directors, said hospital administrators would have to ask Illinois Gov. J.B. Pritzker for help in clarifying state law and whether it permits the policy shift. “It’s a major concern for everyone,” he said. “This is something about which we have had lots of communication with families, and I think they are very aware of the grave circumstances.” Officials at George Washington University Hospital in the District say they have had similar conversations, but for now will continue to resuscitate covid-19 patients using modified procedures, such as putting plastic sheeting over the patient to create a barrier. The University of Washington Medical Center in Seattle, one of the country’s major hot spots for infections, is dealing with the problem by severely limiting the number of responders to a contagious patient in cardiac or respiratory arrest. Several large hospital systems — Atrium Health in the Carolinas, Geisinger in Pennsylvania and regional Kaiser Permanente networks — are looking at guidelines that would allow doctors to override the wishes of the coronavirus patient or family members on a case-by-case basis due to the risk to doctors and nurses, or a shortage of protective equipment, say ethicists and doctors involved in those conversations. But they would stop short of imposing a do-not-resuscitate order on every coronavirus patient. The companies declined to comment. Lewis Kaplan, president of the Society of Critical Care Medicine and a University of Pennsylvania surgeon, described how colleagues at different institutions are sharing draft policies to address their changed reality. “We are now on crisis footing,” he said. “What you take as first-come, first-served, no-holds-barred, everything-that-is-available-should-be-applied medicine is not where we are. We are now facing some difficult choices in how we apply medical resources — including staff.” The new protocols are part of a larger rationing of lifesaving procedures and equipment — including ventilators — that is quickly becoming a reality here as in other parts of the world battling the virus. The concerns are not just about health-care workers getting sick but also about them potentially carrying the virus to other patients in the hospital. R. Alta Charo, a University of Wisconsin-Madison bioethicist, said that while the idea of withholding treatments may be unsettling, especially in a country as wealthy as ours, it is pragmatic. “It doesn’t help anybody if our doctors and nurses are felled by this virus and not able to care for us,” she said. “The code process is one that puts them at an enhanced risk.” Wunderink said all of the most critically ill patients in the 12 days since they had their first coronavirus case have experienced steady declines rather than a sudden crash. That allowed medical staff to talk with families about the risk to workers and how having to put on protective gear delays a response and decreases the chance of saving someone’s life. A consequence of those conversations, he said, is that many family members are making the difficult choice to sign do-not-resuscitate orders. Code blueHealth-care providers are bound by oath — and in some states, by law — to do everything they can within the bounds of modern technology to save a patient’s life, absent an order, such as a DNR, to do otherwise. But as cases mount amid a national shortage of personal protective equipment, or PPE, hospitals are beginning to implement emergency measures that will either minimize, modify or completely stop the use of certain procedures on patients with covid-19. Some of the most anxiety-provoking minutes in a health-care worker’s day involve participating in procedures that send virus-laced droplets from a patient’s airways all over the room. These include endoscopies, bronchoscopies and other procedures in which tubes or cameras are sent down the throat and are routine in ICUs to look for bleeds or examine the inside of the lungs. Changing or eliminating those protocols is likely to decrease some patients’ chances for survival. But hospital administrators and doctors say the measures are necessary to save the most lives. The most extreme of these situations is when a patient, in hospital lingo, “codes.” When a code blue alarm is activated, it signals that a patient has gone into cardiopulmonary arrest and typically all available personnel — usually somewhere around eight but sometimes as many as 30 people — rush into the room to begin live-saving procedures without which the person would almost certainly perish. “It’s extremely dangerous in terms of infection risk because it involves multiple bodily fluids,” explained one ICU physician in the Midwest, who did not want her name used because she was not authorized to speak by her hospital. Fred Wyese, an ICU nurse in Muskegon, Mich., describes it like a storm: A team of nurses and doctors, trading off every two minutes, begin the chest compressions that are part of cardiopulmonary resuscitation or CPR. Someone punctures the neck and arms to access blood vessels to put in new intravenous lines. Someone else grabs a “crash cart” stocked with a variety of lifesaving medications and equipment ranging from epinephrine injectors to a defibrillator to restart the heart. As soon as possible, a breathing tube will be placed down the throat and the person will be hooked up to a mechanical ventilator. Even in the best of times, a patient who is coding presents an ethical maze; there’s often no clear cut answer for when there’s still hope and when it’s too late. In the process, heaps of protective equipment is used — often many dozens of gloves, gowns, masks, and more. Bruno Petinaux, chief medical officer at George Washington University Hospital, said the hospital has had a lot of discussion about how — and whether — to resuscitate covid-19 patients who are coding. “From a safety perspective you can make the argument that the safest thing is to do nothing,” he said. “I don’t believe that is necessarily the right approach. So we have decided not to go in that direction. What we are doing is what can be done safely.” However, he said, the decision comes down to a hospital’s resources and “every hospital has to assess and evaluate for themselves.” It’s still early in the outbreak in the Washington area, and GW still has sufficient equipment and manpower. Petinaux said he cannot rule out a change in protocol if things get worse. GW’s procedure for responding to coronavirus patients who are coding includes using a machine called a Lucas device, which looks like a bumper, to deliver chest compressions. But the hospital has only two. If the Lucas devices are not readily accessible, doctors and nurses have been told to drape plastic sheeting — the 7-mil kind available at Home Depot or Lowe’s — over the patient’s body to minimize the spread of droplets and then proceed with chest compressions. Because the patient would presumably be on a ventilator, there is no risk of suffocation. In Washington state which had the nation’s first covid-19 cases, UW Medicine’s chief medical officer, Tim Dellit, said the decision to send in fewer doctors and nurses to help a coding patient is about “minimizing use of PPE as we go into the surge.” He said the hospital is monitoring health-care workers’ health closely. So far, the percentage of infections among those tested is less than in the general population, which, he hopes, means their precautions are working. ‘It is a nightmare’Bioethicist Scott Halpern at the University of Pennsylvania is the author of one widely circulated model guideline being considered by many hospitals. In an interview, he said a blanket stop to resuscitations for infected patients is too “draconian” and may end up sacrificing a young person who is otherwise in good health. However, health-care workers and limited protective equipment cannot be ignored. “If we risk their well-being in service of one patient, we detract from the care of future patients, which is unfair,” he said. Halpern’s document calls for two physicians, the one directly taking care of a patient and one who is not, to sign off on do-not-resuscitate orders. They must document the reason for the decision, and the family must be informed but does not have to agree. Wyese, the Michigan ICU nurse, said his own hospital has been thinking about these issues for years but still is unprepared. Over the weekend, Wyese said, a suspected covid-19 patient was rushed in and put into a negative pressure room to prevent the virus spread. In normal times, a nurse in full hazmat-type gear would sit with the patient to care for him, but there was little equipment to spare. So Wyese had to monitor him from the outside. Before he walked inside, he said, he would have to put on a face shield, N95 mask, and other equipment and slather antibacterial foam on his bald head as the hospital did not have any more head coverings. Only one powered air-purifying respirator or PAPR was available for the room and others nearby that could be used when performing an invasive procedure — but it was 150 feet away. While he said his hospital’s policy still called for a full response to patients whose heart or breathing stopped, he worried any efforts would be challenging, if not futile. “By the time you get all gowned up and double-gloved the patient is going to be dead,” he said. “We are going to be coding dead people. It is a nightmare.” |
|
“No Hope”: Canada’s Nursing Homes Prepare For Mass Deathby Tyler Durden05April2020 – https://www.zerohedge.com/health/no-hope-canadas-nursing-homes-prepare-mass-death Nursing homes in Canada have been instructed by health officials to ‘keep seniors comfortable’ if they contract COVID-19 and not take them to the hospital due to their high mortality rate, according to Canada’s Global News.
“They’re treating it like a hospice, like there’s no hope like they have stage four brain cancer and they just have to keep them comfortable because there’s nothing they can do,” said Tanya Bartley, whose grandmother died last month at Pinecrest Nursing Home in Bobcaygeon, Ontario – where 22 residents have died and 1/3 of the staff are in isolation due to coronavirus. Community shaken by COVID-19 deaths at Pinecrest Nursing HomeCBC News: The National 31March2020 “They don’t play god. Everybody is the same. I don’t care if it’s a two-year-old, a 10-year-old, a 20-year-old, middle-aged, elderly. I don’t care,” Bartley added. One dementia-stricken resident, Edna Bowers, was one such coronavirus victim who was treated at the home and not transferred to the hospital. In a March 23 letter seen by Global News, Dr. Allan Bell – medical director and chief of emergency medicine at Quinte Health Care (QHC) in Belleville, Ontario, outlines suggestions on how long-term care administrators should prepare for potential COVID-19 outbreaks in their facilities. “Having this conversation pre-emptively is very important. It gives families time to digest the information when they are not in a crisis situation and, should an outbreak happen, it is difficult to manage all of the conversations at once,” reads the letter in part, while also recommending against hospital visits – citing a shortage of medical options for frail patients. “Our critical care colleagues are of the strong opinion that ventilator treatment will not make a survival difference to patients who are frail and ventilator support is very unlikely to be offered,” the letter continues “for those residents who go on to develop respiratory failure, care needs to focus on the provision of comfort to ease suffering at the end of life.” When reached by Global News for comment, Ontario’s Health Minister Christine Elliott said she was unaware of the guidelines – adding that nobody would be denied care in an ER. “If people are ill enough that they have to go to hospital of course they will be transported to hospital. If they’re showing symptoms of COVID-19, they’ve been diagnosed with it but they can be maintained in self-isolation within the home; we’ll do that too but no one is going to be denied health care if they need it,” she said.
According to health officials, residents of long-term care homes are being screened twice daily and are subject to more intense screening in order to try and limit the spread of the virus. New England Journal Paper, Death rates in care homesDr. John Campbell 31March2020 As of March 18th, 30 care facilities with at least one confirmed case of Covid-19 had been identified in King County. CONCLUSIONS INDEX CASE Computed tomographic (CT), diffuse bilateral pulmonary infiltrates. PMH, insulin-dependent type II diabetes mellitus, obesity, chronic kidney disease, hypertension, coronary artery disease, congestive heart failure. Nasopharyngeal and oropharyngeal swabs and a sputum specimen to test for SARS-CoV-2 28 feb, positive result 2 march, patient died on March 2, 2020. |
|
Study: 55% of coronavirus cases in long-term care facilities in Maryland were ASYMPTOMATIC at the time of testing27July2020 by: Arsenio Toledo https://www.naturalnews.com/2020-07-27-majority-of-coronavirus-cases-in-maryland-were-asymptomatic.html< (Natural News) More than half of nursing home residents in Maryland that have tested positive for the Wuhan coronavirus (COVID-19) did not have any symptoms at the time of testing. According to a report by the The New York Times, more than 40 percent of coronavirus-related fatalities in the United States have come from long-term care facilities, such as nursing homes, memory care facilities, assisted-living facilities, rehabilitation centers and retirement and senior communities. Because these facilities have emerged as coronavirus hotspots, a team of researchers from Johns Hopkins University (JHU) set out to determine how the deadly virus was able to spread largely undetected through these institutions. “My thought in doing this is that we had an opportunity in the nursing home setting to be South Korea – to provide widespread testing, really identify the burden of disease and then try to isolate based on that,” said Morgan Katz, one of the authors of the study and an assistant professor of medicine at JHU’s School of Medicine. Katz and her colleagues decided to study nine nursing homes and two assisted-living facilities in Maryland that had confirmed COVID-19 cases. Initially, these facilities had 153 cases that were identified through targeted, symptom-based testing. When the researchers tested the remaining 893 residents, they found an additional 354 cases of COVID-19, which meant that more than half of the residents in these 11 long-term care facilities had the coronavirus. According to the study, around 55 percent of all the infected residents were asymptomatic at the time of testing. Many of these positive residents developed serious illnesses soon afterward. Katz’s team followed up on seven of the facilities after two weeks and found that 20 of the 154 then-asymptomatic patients required hospitalization, while seven passed away due to COVID-19 complications. Katz believes their research highlights the necessity of following the guidelines set by the the Centers for Disease Control and Prevention (CDC), which require all residents and staff members of nursing homes to be tested if even one positive case is found. Unfortunately, the federal government only requires facilities to report infections and deaths and does nothing but offer recommendations on how often they should conduct COVID-19 tests on their residents. Many states have different policies on testing nursing home workers, and some states like California are beginning to reopen even their nursing homes to allow visitors to come and go. Katz believes that this policy reduces the efficacy of one-time baseline testing, and what these facilities need are “on-site tests with rapid turnaround times so they really can respond immediately to any potential outbreaks.” (Related: Cuomo claims nursing home outbreaks spread by workers, not his directive that FORCED facilities to bring in more coronavirus patients.) Watch this episode of Brighteon Conversations with Mike Adams, the Health Ranger, as he has a very engaging and illuminating discussion with Dr. Paul Cottrell about a new strain of the Wuhan coronavirus known as “D614G,” which spreads a lot more easily than older variants of COVID-19. Dr. Paul Cottrell warns of new coronavirus mutation that spreads more easilyOne Maryland nursing home able to repel the coronavirus by acting quickly and locking down the facilityWhile many long-term care institutions in Maryland have to deal with rising COVID-19 cases within their facilities, the Maryland Baptist Aged Home in Baltimore has not reported a single case of infection since the beginning of the outbreak in America. The head of the facility, Rev. Derrick DeWitt, said that the key to his nursing home’s success was early mitigation, and the application of proactive protocols that prevented the coronavirus from entering. Back in February when the U.S. only had around 15 cases, the nursing home sprung into action before the rest of the country even began locking down. On March 1, the nursing home went into a full lockdown. Visitors were not allowed to enter the facility, and they instituted a very thorough, rigorous screening process for their employees, which included providing the facility with the details of where the workers were during their time off, the regular taking of body temperatures and the wearing of protective gear – masks, gowns and gloves – whenever they had to come into contact with any of the home’s residents. Maryland Baptist also benefited from the fact that DeWitt hired a full-time quality assurance and infection control nurse who set up many of the anti-coronavirus measures the facility greatly benefited from. Lastly, DeWitt cared for the emotional well-being of his residents by bringing in extra activity staff who made sure that the residents had visitors to interact with on a daily basis. He even hired a chef who came to help his staff prepare the residents’ meals and make them more pleasing. The story of Maryland Baptist and Rev. DeWitt’s quick response to the pandemic shows how institutions can keep the coronavirus outside of their walls. Maryland Baptist’s success is a bright spot in the otherwise bleak events that have affected nursing homes all across the country. According to The New York Times, at least 296,000 residents in long-term care facilities have contracted the coronavirus, and 55,000 have died. If long-term care facilities learn from Maryland Baptist’s example and apply Katz’s recommendation to conduct regular and rapid COVID-19 testing on nursing home employees and residents, future fatalities in many nursing homes could be prevented. Learn about how other institutions are fighting back against the coronavirus by reading the articles at Pandemic.news. Sources include: |
|
Bombshell plea from NYC ICU doctor: COVID-19 is a condition of oxygen deprivation, not pneumonia… VENTILATORS may be causing the lung damage, not the virus04April2020 by: Mike Adams https://www.naturalnews.com/2020-04-04-nyc-icu-doctor-covid-19-oxygen-deprivation-not-pneumonia-ventilators.html (Natural News) A NYC physician named Cameron Kyle-Sidell has posted two videos on YouTube, pleading for health practitioners to recognize that COVID-19 is not a pneumonia-like disease at all. It’s an oxygen deprivation condition, and the use of ventilators may be doing more harm than good with some patients. The ventilators themselves, due to the high-pressure methods they are running, may be damaging the lungs and leading to widespread harm of patients. Dr. Cameron Kyle-Sidell describes himself as an “ER and critical care doctor” for NYC. “In these nine days I have seen things I have never seen before,” he says. Before publishing his video, we confirmed that Dr. Kyle-Sidell is an emergency medicine physician in Brooklyn and is affiliated with the Maimonides Medical Center located in Brooklyn. In his video (see below), he goes on to warn the world that the entire approach to treating COVID-19 may be incorrect, and that the disease is something completely different from what the dogmatic medical establishment is claiming. “In treating these patients, I have witnessed medical phenomena that just don’t make sense in the context of treating a disease that is supposed to be a viral pneumonia,” he explains. He talks about how he opened a critical care using expecting to be treating patients with a viral pneumonia infection that would progress into Acute Respiratory Distress Syndrome (ARDS). But that the disease acted nothing like ARDS. “This is the paradigm that every hospital in the country is working under,” he warns. “And yet, everything I’ve seen in the last nine days, all the things that just don’t make sense, the patients I’m seeing in front of me, the lungs I’m trying to improve, have led me to believe that COVID-19 is not this disease, and that we are operating under a medical paradigm that is untrue.” More from Dr. Kyle-Sidell: (emphasis added) In short, I believe we are treating the wrong disease, and I fear that this misguided treatment will lead to a tremendous amount of harm to a great number of people in a very short time… I feel compelled to give this information out. COVID-19 lung disease, as far as I can see, is not a pneumonia and should not be treated as one. Rather, it appears as if some kind of viral-induced disease most resembling high altitude sickness. Is it as if tens of thousands of my fellow New Yorkers are on a plane at 30,000 feet at the cabin pressure is slowly being let out. These patients are slowly being starved of oxygen. And while [patients] absolutely look like patients on the brink of death, they do not look like patients dying from pneumonia… I suspect that the patients I’m seeing in front of me, look as if a person was dropped off on the top of Mt. Everest without time to acclimate. He goes on to explain that ventilators, in some cases, may be doing far more harm than good. When we treat people with ARDS, we typically use ventilators to treat respiratory failure. But these patients’ muscles work fine. I fear that if we are using a false paradigm to treat a new disease, then the method that we program [into] the ventilator, one based on respiratory failure as opposed to oxygen failure, that this method being widely adopted … aims to increase pressure on the lungs in order to open them up, is actually doing more harm than good, and that the pressure we are providing to lungs, we may be providing to lungs that cannot take it. And that the ARDS that we are seeing, may be nothing more than lung injury caused by the ventilator. There are hundreds of thousands of lungs in this country at risk. In other words, the real disease appears to cause oxygen deprivation in victims, not pneumonia. This is critically important for all the obvious reasons, and it raises huge questions about the origins of the coronavirus and whether there is some additional external factor beyond the virus that may be causing a combined effect that results in severe oxygen deprivation. FROM NYC ICU: DOES COVID-19 REALLY CAUSE ARDS??!!Cameron Kyle-Sidell 31March2020
Watch this second video where he begs the world to recognize that the ventilator protocols are not working and must be changed. From this second video: We don’t know where we’re going. We are putting breathing tubes in people and putting them on ventilators and dialing up the pressure to open their lungs. I’ve talked to doctors all around the country and it is becoming increasingly clear that the pressure we are providing may be hurting their lungs. That it is highly likely that the high pressures we are using are damaging the lungs of the patients we are putting breathing tubes in… we are running the ventilators in the wrong way…. COVID-19 patients need oxygen, they do not need pressure. FROM NYC DOC: SHOULD COVID-19 VENTILATOR PROTOCALS BE CHANGED!!!Cameron Kyle-Sidell 01April2020 |
|
Overreliance on ventilators led to coronavirus deaths, study shows06June2020 by: Franz Walker https://www.naturalnews.com/2020-06-06-overreliance-on-ventilators-coronavirus-deaths.html (Natural News) The use of ventilators to treat COVID-19 patients has come under scrutiny after a new study stated that the devices may be doing more harm than good. The study, published in the American Journal of Tropical Medicine and Hygiene, said that mechanical ventilation can damage the lungs of COVID-19 patients, especially those who are elderly or have severe symptoms. This means that healthcare professionals will have to re-evaluate their reliance on ventilators for these patients and stop being so quick to intubate. “This is one of the first coherent, comprehensive, and reasonably clear discussions of the pathophysiology of Covid-19 in the lungs that I’ve seen,” said Dr. Muriel Gillick, a palliative care physician at Harvard Medical School who was not involved with the study. Gillick was among the experts who questioned the effectiveness of ventilators in COVID-19 patients, according to STAT. High-pressure oxygen damages the lungsThe reason why intubation and mechanical ventilation damages the lungs of very ill and elderly patients could be down to a poorly understood function of the disease, which behaves differently than other respiratory illnesses. The lungs of COVID-19 patients with severe symptoms are often covered with thick mucus. This prevents the lungs from being able to absorb oxygen, even with the use of a ventilator. In addition, unlike other types of pneumonia, the areas of lung damage in COVID-19 patients often sit right next to healthy tissue. When large volumes of oxygen-rich air are forced into the elastic at high pressures, it can lead to what the study calls “ventilator-induced injury.” These injuries include leaks, inflammation and blood clots in the lungs. “Invasive ventilation can be lifesaving, but can also damage the lung,” co-author Marcus Schultz told STAT. Patients with low levels of blood oxygen don’t necessarily require ventilationMost healthcare professionals tend to use hypoxemia — having abnormally low levels of oxygen in the blood — as a sign that a patient needs mechanical ventilation. But, as the researchers pointed out, equating hypoxemia to the need for a ventilator can lead healthcare workers astray. While the team agrees that a patient who is clearly struggling to breathe should be intubated, they noted that hypoxemia in COVID-19 patients manifests differently than with other diseases like other forms of pneumonia or sepsis. For non-COVID-19 patients exhibiting hypoxemia, they often gasp for air and can barely speak. However, coronavirus patients — even those with blood oxygen levels at 80 percent or lower — can speak full sentences without getting winded. In addition, these patients don’t show the usual signs of respiratory distress associated with hypoxemia. For comparison, normal blood oxygen levels are in the high 90s. “In our personal experience, hypoxemia … is often remarkably well tolerated by Covid-19 patients,” the researchers wrote. “The trigger for intubation should, within certain limits, probably not be based on hypoxemia but more on respiratory distress and fatigue.” Without any signs of distress, the researchers state that the blood oxygen levels of coronavirus patients don’t need to be raised above 88 percent. This is a much lower level than in other causes of pneumonia. University of California, San Francisco’s Phil Rosenthal, editor of the journal, agreed with the researchers, stating that it was important to highlight “aspects of COVID-19 that differ from other diseases that require respiratory support.” He said that recognizing the difference in how COVID-19 patients respond to low blood oxygen levels compared to patients of other illnesses “may allow physicians to avoid intubation/ventilator support in some patients.” There is a growing recognition that coronavirus patients, even those with a severe lung infection, can be treated safely with simple face masks and nose prongs that deliver oxygen. The former include continuous positive airway pressure (CPAP) masks often used for patients with sleep apnea, or biphasic positive airway pressure masks (BiPAP) used for those with congestive heart failure. CPAP can also be delivered using hood or helmets, reducing the risk that the patient will expel large quantities of the virus into the air and endanger healthcare workers and other patients. In addition, in the face of ventilator shortages, switching to CPAP and BiPAP masks can allow healthcare systems to keep ventilators in reserve for those patients who do need them. Visit Pandemic.news to learn more about COVID-19. Sources include: Nurses Are Beginning to Come ForwardSomething Feels Wrong 4May2020 |
|
Coronavirus hijacks immune cells to create cytokine storms, says new study27May2020 by: Ralph Flores https://www.naturalnews.com/2020-05-27-coronavirus-hijacks-immune-cells-to-create-cytokine-storms.html (Natural News) Scientists continue to be baffled by the Wuhan coronavirus (COVID-19), especially how it “hijacks” certain cells of the body. A new study from the Icahn School of Medicine at Mount Sinai suggests that SARS-CoV-2 – the coronavirus strain behind the current pandemic – can inhibit one virus-fighting set of genes but allow another set to launch – a pattern not seen with other viruses. For Benjamin tenOever, a virus expert at Mount Sinai and the senior author of the study, this behavior is something he has not seen in his 20 years of studying viruses. Other viruses, like the flu virus and the original SARS virus, interfere with two sets of genes in the body’s immune response: The one that prevents viruses from replicating and the other that recruits immune cells to the infection site to kill viruses. The first group of genes, which tenOever dubs “call to arms genes,” produces interferons, which are proteins that interfere with the virus’s ability to replicate. These proteins are important modulators of the immune response. Once interferons are released, they serve as a signal to nearby cells to activate their own genes. This slows down the virus’s ability to make copies of itself if it invades them. According to tenOever, this process lasts anywhere between seven to 10 days, which is plenty of time for the second group of genes to do their job. The second group of genes produces chemokines, which are small proteins that emit a biochemical “come here!” alarm. TenOever calls these “call for reinforcement” genes, on account that other immune cells – like the antibody-making B cells and the virus-killing T cells – rush to chemokine sources once they sense the alarm. “Most other viruses interfere with some aspect of both the call to arms and the call for reinforcements,” tenOever added. “If they didn’t, no one would ever get a viral illness.” SARS-CoV-2, however, behaves differently. It prevents the first group of genes from producing interferons that can slow its replication but allows the second group of genes to secrete chemokines. This not only allows the virus to multiply unchecked, but it also causes immune cells to flood the lungs. The result is a storm of inflammatory molecules in the affected organ, which tenOever calls a unique and aberrant consequence of SARS-CoV-2. When your immunity turns against youTenOever and his team examined healthy lung cells growing in lab dishes, ferrets (which they called an appropriate animal model for SARS-CoV-2 infections) and lung cells from coronavirus patients. Within three days of infection, the team found a mild response from the “call to arms” genes that inhibit replication and a large introduction of the “call for reinforcement” genes. “Basically people are contracting the disease, SARS-CoV-2 enters the lungs and it begins to replicate and, at that site of replication, those cells that are infected, they don’t do a good job of spreading the word about their infection which allows it to essentially fester in the lungs,” tenOever explained. Without interferons, the virus is free to infect other cells and replicate much faster, all while cells in the area continue to call for reinforcements. But by the time the reinforcements arrive, the virus has grown out of control. The presence of large amounts of immune cells, on the other hand, triggers uncontrolled levels of inflammation, which does nothing but induce more inflammation. This could explain why people with COVID-19 experience “cytokine storms” in which the body attacks its own cells and tissues instead of just the virus. (Related: Study: Vitamin D deficiency found to increase the risk of fatal coronavirus infections and a deadly “cytokine storm.”) According to tenOever, their findings point to two methods of treatment. For patients who have just started developing symptoms, he says that therapy should focus on inducing the missing “call to arms” genes, so the virus can behave similarly to that of the flu. But for those with severe symptoms, he says that reducing inflammation and the risk of cytokine storms will be beneficial. TenOever and his team’s findings were published last week in the journal Cell. Pandemic.news has the latest on the ongoing coronavirus outbreak. Sources include: |
|
Lancet Issues Major Disclaimer On Anti-HCQ Study, As Manufactured Disinformation Foments Hystericsby Tyler Durden 02June2020 https://www.zerohedge.com/markets/exposing-manufactured-disinformation-enabling-hydroxychloroquine-hysterics The Lancet has issued a major disclaimer regarding a study which prompted the World Health Organization to halt global trials of hydroxychloroquine (HCQ), an anti-Malaria drug currently being used around the world to treat COVID-19. As we noted last week, major data discrepancies have called the entire study into question – though the lead author says it does not change the study’s findings that patients who received HCQ died at higher rates and experienced more cardiac complications than without. Until the data has been audited, The Lancet issued the following “expression of concern” regarding the study.
Of course, this is yet more evidence of the manufactured disinformation surrounding HCQ that Richard Moss, MD, (via AmericanThinker.com) exposes below… I took hydroxychloroquine for two years. A long time ago as a visiting cancer surgeon in Asia, in Thailand, Nepal, India, and Bangladesh. From 1987 to 1990. Malaria is rife there. I took it for prophylaxis, 400 milligrams once a week for two years. Never had any trouble. It was inexpensive and effective. I started it two weeks before and was supposed to continue it through my stay and four weeks after returning. But I stopped it after two years. I was worried about potential side effects of which there are many, as with all drugs right down to Tylenol and aspirin. These, however, are rare. At a certain point, I was prepared to take my chances with mosquitoes and plasmodium, and so I stopped. Chloroquine, the precursor of HCQ, was invented by Bayer in 1934. Hydroxychloroquine was developed during World War II as a safer, synthetic alternative and approved for medical use in the U.S. in 1955. The World Health Organization considers it an essential medicine, among the safest and most effective medicines, a staple of any healthcare system. In 2017, US doctors prescribed it 5 million times, the 128th most commonly prescribed drug in the country. There have been hundreds of millions of prescriptions worldwide since its inception. It is one of the cheapest and best drugs in the world and has saved millions of lives. Doctors also prescribe it for Lupus and Rheumatoid arthritis patients who may consume it for their lifetimes with few or no ill effects. Then something happened to this wonder drug.
 Hydroxychloroquine
From savior of the multitudes, redeemer and benefactor of hundreds of millions, it transformed into something else: a purveyor of doom, despair, and unspeakable carnage.
 Hydroxychloroquine and Trump
It began when President Trump discussed it as a possible treatment for COVID-19 on March 19, 2020. The gates of hell burst forth on May 18 when Trump casually announced that he was taking it, prescribed by his physician. Attacks on Trump and this otherwise harmless little molecule poured in. The heretofore respected, commonly used, and highly effective medicinal became a major threat to life, a nefarious and wicked chemical that could alter critical heart rhythms, resulting in sudden cataclysmic death for unsuspecting innocents. Trump, more than irresponsible, was evil incarnate for daring to even mention it. While at it, the salivating media trotted out the canard about Trump’s nonrecommendation for injecting Clorox and Lysol or drinking fish-tank cleaner to combat COVID. It was Charlottesville all over again. Before a nation of non-cardiologists, the media agonized over, of all things, the prolongation of the now infamous “QT interval,” and the risk of sudden cardiac death. The FDA and NIH piled on, piously demanding randomized, controlled, double-blind studies before physicians prescribed HCQ. No one mentioned that the risk of cardiac arrest was far higher from watching the Superbowl. Nor did the media declare that HCQ and chloroquine have been used throughout the world for half a century, making them among the most widely prescribed drugs in history with not a single reported case of “arrhythmic death” according to the sainted WHO and the American College of Cardiology. Or that physicians in the field, on the frontlines, so to speak, based on empirical evidence, have found benefit in treating patients with a variety of agents including HCQ, Zinc, Azithromycin, Quercetin, Elderberry supplements, Vitamins D and C with few if any complications. Or that while such regimens may not cure, they may help and carry little or no risk. And so, the world was aflame once again with a nonstory driven by the COVID media. The HCQ divide within the nation is only a continuation of innumerable divides that have surfaced since the pandemic began — and before. One will know the politics of an individual based on his position on any number of pandemic issues: lockdowns, sheltering in place, face masks, social distancing, “elective surgery,” and “essential businesses.” The closing of schools and colleges. Blue states and Red states. Governor Cuomo or Governor DeSantis. Nationwide injunctions or federalism. The WHO and Red China. Or, pre-pandemic, Brexit, open borders, DACA, and amnesty. CBD oil, turmeric, and legalizing marijuana. Russia Collusion, Trump’s taxes, the 25th amendment, Stormy Daniels, the Ukraine non-scandal, and impeachment. Or Obamagate. And now HCQ. HCQ is only another bellwether. It represents the latest nonevent in a long string of fabricated media nonscandals. If a nation can be divided over HCQ it can be divided over anything. It shows neatly, as many of the other non-issues did, whether one embraces the U.S., our history, culture, and constitutional system, or rejects it. Whether one believes in Americanism or despises it. It is part of the ongoing civil war, thus far cold, but who knows? The passions today are no less jarring than they were in 1860. One would have thought that a man taking a medicine prescribed by his physician, even a President, would be a private matter. But no. Not today. We swim in an ocean of manufactured disinformation created by a radical COVID media, our fifth column. They inflame the nation one way or another based on political whims. The propaganda arm of the Left, they seek victory at all costs including dismantling the economy, culture, and our governing system. Is there a curative for the COVID media and their Democrat allies who would destroy a nation to destroy Trump? He is all that stands between us and them. Is there an antiviral for this, the communist virus that has infected the nation, metastasized throughout its corpus, and now threatens the republic? * * * Dr. Moss is a practicing Ear Nose and Throat Surgeon, author, and columnist, residing in Jasper, IN. He has written A Surgeon’s Odyssey and Matilda’s Triumph available on amazon.com. Find more of his essays at richardmossmd.com. |
|
COVID-19 vaccine trial participant DIES… AstraZeneca downplays the death and continues the medical experiments on the remaining humansThursday, October 22, 2020 by: Mike Adams https://www.naturalnews.com/2020-10-22-covid-19-vaccine-trial-participant-dies-astrazeneca.html (Natural News) A person who volunteered for the medical experimentation on humans with the COVID-19 vaccine has died during clinical trials, reports The Epoch Times. The death was confirmed by government officials in Brazil, where the trial was taking place, and the company whose vaccine is being tested in the medical experiments — AstraZeneca — says it will continue its experiments on the remaining human survivors. No deaths will stand in the way of vaccine profits, it seems. “The volunteer died on Oct. 15,” reports The Epoch Times. “It’s not clear whether the volunteer received the placebo shot or the vaccine.” Had this person died in any other context, their death would of course have been counted as a “covid-19 death,” but since they are involved in a vaccine trial, the scheming mainstream media will claim the person received a placebo, not a live vaccine. Such claims are complete fiction, given that no such patient data are allowed to be released on individual patients. As TET reports: The health authority noted that “data on clinical research volunteers must be kept confidential, in accordance with the principles of confidentiality, human dignity, and protection of participants,” according to a news release. Thus, any media outlet reporting the vaccine trial participant was part of the placebo group is lying. Then again, all they do is lie. The human medical experiments continue, no matter how many die in the process“We cannot comment on individual cases in an ongoing trial of the Oxford vaccine as we adhere strictly to medical confidentiality and clinical trial regulations, but we can confirm that all required review processes have been followed,” said AstraZeneca in a public statement. This isn’t the first indication of dangerous side effects linked to coronavirus vaccines. “It came after AstraZeneca said on Sept. 8 that its vaccine trial was placed on hold due to an illness in a patient in the United Kingdom,” reports TET. “The Food and Drug Administration placed a late-stage clinical trial from AstraZeneca on hold in the United States.” Just yesterday, Natural News reported how Johnson & Johnson was forced to halt another coronavirus vaccine trial after a trial participant experienced an “unexplained illness.” As that story explains: Johnson & Johnson is pausing its Wuhan coronavirus (COVID-19) vaccine trial after a study participant fell ill. The halt comes just weeks after the company announced that they were in the final stage of the trials. In its news release, Johnson & Johnson said that the trial was paused in compliance with regulatory standards after the unnamed participant developed an “unexplained illness.” In related news, nine people have died in South Korea after receiving flu shots there, causing a nationwide panic over the “death vaccines” that are killing so many people so quickly. As Strange Sounds reports: Nine people have died after getting flu shots in South Korea in the past week, raising concerns over the vaccine’s safety just as the seasonal inoculation programme is expanded to head off potential COVID-19 complications. Health authorities there are saying the vaccines didn’t kill anyone, since the dead people had “underlying health conditions,” which is exactly what Natural News warned would be said about vaccine deaths as the body count started to accelerate. Notably, when people with underlying health conditions die with a coronavirus infection, they are said to have died from covid-19. But when they have underlying health conditions and are found dead after receiving a vaccine injection, health authorities claim the vaccine isn’t related to their death. How convenient. Operation Fast KillIt all begs the question: If human volunteers are now starting to die during the carefully controlled trials that recruit extremely healthy individuals for testing, what’s going to happen when these risky, rushed vaccines are unleashed upon the wildly unhealthy general public? Operation Warp Speed is about to become Operation Fast Kill, it seems. Then again, there’s no faster way for globalists to exterminate people who are too stupid to realize the covid-19 agenda is actually an extermination agenda targeting the human race. On the other hand, those who are intelligent enough to want to survive should be steering clear of all vaccines and vaccine industry medical experiments carried out on humans. Obviously. Dr. Carrie Madej warns us all about the dangerous of coronavirus vaccines. Check out her video channel on Brighteon.com: Brighteon.com/channels/drcarriemadej Dr. Carrie Madej warns about coronavirus vaccines and transhumanism nanotechnology to alter your DNAAnd follow my real-time news reports and commentary at Brighteon.social, the new free speech alternative to Facebook and Twitter. Over 13,000 users are there already, and they are truly enjoying being able to speak freely, without Big Tech censorship. Also see VaccineDeaths.com for more reporting on how vaccines are killing people. |
|
Health systems collapsing around the country as L.A. County orders EMS not to transport patients who have “little chance” to surviveWednesday, January 13, 2021 by: JD Heyes https://www.naturalnews.com/2021-01-13-la-county-orders-ems-not-transport.html (Natural News) Health systems in America are under so much strain as new COVID-19 infections rise that emergency medical services in some parts of the country are being overwhelmed. For instance, health officials in Los Angeles County have instructed ambulance crews not to transport any patients who have “little chance of survival,” The Epoch Times reported last week. A directive from the Los Angeles County Emergency Medical Services Agency dated Jan. 4 instructs EMS personnel to also cut back on the use of oxygen throughout L.A. County, the most populous in all of California, which currently has a virus infection rate of 138 per 100,000 people, according to the state’s tracking system. “Oxygen for the purposes of medication administration and CPAP may be used when needed,” the directive states, adding that patients with an O2 saturation of 90 percent or less should receive it. “An oxygen saturation of 90% is sufficient to maintain normal tissue perfusion in most patients,” the directive adds. The EMS agency noted further that “titrated oxygen with a higher target of 94% is recommended for the following specific conditions: carbon monoxide poisoning, suspected pneumothorax, shock, traumatic brain injury.” The agency also noted that because of a serious shortage of hospital ICU beds in the county, EMS crews should not be transporting patients if they have suffered cardiopulmonary arrest and attempts to revive them have not been successful, the Los Angeles Times reported. Before the pandemic, EMS crews typically transported patients to hospitals even if they had little-to-no-chance of pulling through. At the present time, “many hospitals have reached a point of crisis and are having to make very tough decisions about patient care,” Dr. Christina Ghaly, director of L.A. County health services, told reporters earlier this month. “The volume being seen in our hospitals still represents the cases that resulted from the Thanksgiving holiday,” she added during a briefing Monday. “We do not believe that we are yet seeing the cases that stemmed from the Christmas holiday. This, sadly, and the cases from the recent New Year’s holiday, is still before us, and hospitals across the region are doing everything they can to prepare.” Besides EMS, hospitals are also adopting new policies aimed at opening up beds more quickly. Some sick patients are being discharged, for instance, though under normal circumstances they would remain in the hospital for continued observation. (Related: Liberal states facing a COLLAPSE of state incomes thanks to coronavirus shutdowns: Will pensions collapse, too?) The LA Times adds: Emergency rooms are so slammed that some patients are having to wait inside ambulances for as long as eight hours before a bed becomes available. That backlog ties up ambulances and keeps them from being able to respond to other emergency calls. To deal with the shortage, officials have devised an emergency plan to create temporary “ambulance-receiving spaces” — set up just outside the emergency room entrance and often covered by tents or canopies — to accept patients. Paramedics and EMTs may also be utilized to help monitor up to four patients at once in receiving spaces, which is different from the previous policy of one-on-one monitoring. This allows more ambulances to be freed up to respond to other calls. “We’re likely to experience the worst conditions in January that we’ve faced the entire pandemic, and that’s hard to imagine,” said L.A. County Public Health Director Barbara Ferrer, the Times reported. As such, the number of Wuhan coronavirus patients who have to be hospitalized will continue spiking “as long as our case numbers increase,” she said in a briefing. “Everyone should keep in mind that community transmission rates are so high that you run the risk of an exposure whenever you leave your home,” Ferrer said. “Assume that this deadly, invisible virus is everywhere, looking for a willing host. Don’t let that be you or someone you care about.” See more reporting like this at Pandemic.news. Sources include: |
|
COVID Lockdowns Will Result In 1 Million Excess Deaths Over Next 15 Years, Scientists Findby Tyler Durden Back in the summer of 2020, a critical discussion almost broke out between progressives on one hand, who were adamant that if “just one life” could be saved with pervasive, widespread economic lockdowns that it was everyone’s imperative to bring the economy to a crawl, and pragmatic, rational thinkers who argued that the economic cost of such lockdowns would end up being far greater than the immediate human cost in terms of lives lost, especially since the impacted lives would be far younger than potential covid vicitms most of whom are in their 70s and 80s. Deutsche Bank credit strategist Jim Reid summarized it best as follows:
Reid then argued that since “younger people will be suffering most from the economic impact of Covid-19 for many years to come, we wonder how history will judge the global response.” To this, however, we countered that since the economic crisis resulting from Covid-19 helped crush Donald Trump’s chances for re-election and also unleashed full-blown helicopter money as well as the biggest round of corporate bailouts of insolvent and zombie companies in history, “we are confident that the tsunami of global moral hazard – which will leave tens of millions of young workers without a job – will allow central bankers to sleep soundly at night.” Unfortunately as we said at the top, this discussion “almost” happened, although in the end it did not because any time an attempt for rational discourse emerged it would be promptly and violently shouted down by the armies of virtue signalers who were also monetarily incentivized in maintaining the lockdown status quo (such as bankers, pharma and online payment companies, politicians, the media and so on) and who would instantly defer to the “scientists” as the only expert class worth opining on the critical debate of “excess covid deaths now” vs “excess deaths from economic shutdowns later.” Well, with a roughly one year delay, scientists from Duke, Harvard, and Johns Hopkins finally wrote a paper which may come as a shock to all the virtue-signaling progs out there, because its conclusion is stunning: in a nutshell, the NBER working paper (“The Long-Term Impact Of The Covid-19 Unemployment Shock On life Expectancy And Mortality Rates“) finds that while there have been roughly 400,000 covid-linked deaths so far (amid extensive debate of just what is a “covid-linked death” since even crash victims are counted as covid casualties, not to mention tens of thousands of others with terminal co-morbidities), the long-term economic implications from covid-related lockdowns are dire, resulting in COVID-19-related unemployment “which is between 2 and 5 times larger than the typical unemployment shock” and resulting in a “3.0% increase in mortality rate and a 0.5% drop in life expectancy over the next 15 years for the overall American population.” The bottom line, as scientists Bianchi, Bianchi and Song find is that…
That’s bad; where it gets even worse for the world’s progressives is the report’s finding that the “shock will disproportionately affect” women, particularly of Hispanic heritage; African Americans; foreign born individuals; less educated adults and individuals age 16-24 – in short all those racial and social classes that are of primary concern to the “progressives” – while “white men might suffer large consequences over longer horizons” (we doubt progs will care too much about this). In short, everyone will be hit by the covid-lockdowns, with blacks, Hispanics and women first, and white men next for a far longer period of time. And, in the process, nearly 1 million excess deaths will take place that wouldn’t have taken place otherwise. We wonder how those same progressives, who demanded wholesale economic lockdowns – because that’s the only way to save even one life – will feel now that scientists explicitly state that their preferred policies will lead to nearly a million excess deaths simply from the economic shutdowns. Or, as Reid warned all the way back in July 2020 – when nobody bothered to listen – “younger people will be suffering most from the economic impact of Covid-19 for many years to come, we wonder how history will judge the global response.” Here are some more details from the NBER paper:
Which merely goes to show just how idiotic macroeconomics as a so-called “science” truly is, because if economists are truly baffled by this “shortcoming”, maybe they should take a look at the millions of small businesses and unemployed service workers to emerge from the covid crisis. Anyway, continuing with the paper:
We fast-forward to the conclusion:
And the damning piece de resistance which every virtue signaler will rush to burn before reading
Needless to say, the longer the lockdowns continue, the death toll will only grow bigger across all races and social classes. But wait, there’s even more! As we reported last week, a new peer reviewed study out of Stanford has questioned the effectiveness of lockdowns and stay-at-home orders (which it calls NPIs, or non-pharmaceutical interventions) to combat Covid-19. The study’s lead author (an associate professor in the Department of Medicine at Stanford), found that “the study did not find evidence to support that NPIs were effective in preventing the spread” and that “we fail to find strong evidence supporting a role for more restrictive NPIs in the control of COVID in early 2020.” So, did left-leaning states’ rushed policies in response to the pandemic – to unleash broad lockdowns, crush economies, and spark mass unemployment and poverty leading to increasing deaths of despair actually achieve anything? The short answer is no… California vs Florida covid lockdowns
… while the longer answer we now know thanks to the NBER report, is yes: they made the situation for African Americans, Hispanics and women (and yes, even white men) considerably worse for at least the next two decades. In other words, while lockdowns may not have even led to a tangible improvement in halting the spread of covid, what they will certainly do is lead to hundreds of thousands, perhaps millions, in excess deaths over the next decade. Which begs the question: now that “respected scientists” have finally quantified the “staggering” excess death toll resulting from covid lockdowns, is it time to finally have the discussion – which nobody has dared to have since about a year ago – about the cost-benefit analysis between widespread economic lockdowns, which will lead over a million early deaths, and locking down the economy every time there is even a modest rebound in covid cases…  covid flowchart
… as per the covid we created several months ago, and which may have zero positive impact on actually halting the spread of covid? |
|
California’s Continuing Responses to COVID-19 Pandemic are Full of Failure at All LevelsPosted by Leslie Eastman Wednesday, February 3, 2021 https://legalinsurrection.com/2021/02/californias-continuing-responses-to-covid-19-pandemic-are-full-of-failure-at-all-levels/ Failure highlights: “Hero Pay” store closures, TV-free Super Bowl, and a chaotic vaccination program.I have written about California Governor Gavin Newsom’s recall challenge, partly from the harsh pandemic restrictions that he ignored when convenient.
However, there is much failure at all levels in the Golden State. For example, Kroger, the parent company of Ralphs and Food 4 Less, announced that it is closing two of its stores in Long Beach due to city officials imposing a “hero pay” increase of $4 per hour for some workers.
Another virtue-signaling rule imposed by local officials hurts the very citizens they swore to serve. The Los Angeles County Board of Supervisors has moved forward with a similar proposal for stores in unincorporated parts of the county.
 Kevin de Leon-tweet-2Febuary2021- For the past year, grocery store workers remained on the front lines of the pandemic while COVID decimated cities across the nation. Today I voted to ensure #HeroPay (addt’l $5/hr) to these dedicated workers who continue to put their lives on the line for all of us. #hazardpay
When it comes to mandates, no aspect is too trivial for California bureaucrats. Just as they approved outdoor dining and Americans prepare for the Super Bowl, restaurants and bars won’t be able to bring out the big screen TV.
 Talk-Radio-105.9-tweet-2Febuary2021 It’s a ritual of dining out to look out for the big screen televisions to keep updated on the Lakers score or monitor the NFL or soccer, even if your occasion is celebrating Mom’s birthday or closing a business deal.
Finally, analysis of the California COVID-19 vaccination program shows that it lags behind other large states.
 Angela Hart-tweet-29January2021 CA Gov Newsom recall
California: Come for the sunshine and beaches, stay for the struggles and disease. |
|
15 States Are Moving To Curb Public Health Agency Powers Following Lockdown Carnageby Tyler Durden 15June2021 – https://www.zerohedge.com/markets/15-states-are-moving-curb-public-health-agency-powers-following-lockdown-carnage Authored by John Miltimore via The Foundation for Economic Education, More than a dozen states have passed or advanced legislation to place new checks on the powers of public health agencies in the wake of the pandemic…
 Covid-19 Lockdown business closed
Mike Fratantuono grew up in a restaurant. Literally. For decades, Sunset Restaurant in Glen Burnie, Maryland, was the family business. Over the years, he’d done seemingly every job imaginable: busboy, bartender, and butcher; prep cook and plumber; handyman and manager. Fratantuono says that’s what made it so hard to watch the family’s legacy become a COVID casualty in 2020.
Fratantuono is just one of the countless business owners across America who saw their dreams vanish before their eyes in the wake of government lockdowns that crushed their businesses. Now, in the wake of the pandemic, states across the country are advancing legislation to curb the powers of public health departments following one of the most destructive and contentious years in American history. Reining in Public Health AgenciesIn May, the Network for Public Health Law published a report showing that in recent months no fewer than 15 state legislatures have passed or are considering passing measures that would restrict the legal authority of public health departments. Among the provisions passed or considered are the following:
Earlier this year, for example, North Dakota passed legislation making it unlawful for state officials to force citizens to wear masks—just one of a growing number of states to place restrictions on mask orders. In March, Kansas’s legislature passed legislation that removes the governor’s ability to shut down businesses during a public health emergency. Meanwhile, more than 40 states passed legislation that made it unlawful for health departments to mandate COVID-19 vaccination.
 Jon Miltimore-tweet-9June202115 A recent report found that no fewer than 15 state legislatures have passed or are considering passing measures that would curb the powers of public health departments. A Serious Threat to Life?The report concludes that opposition to “reasonable” public health measures poses serious dangers to life and health.
Not mentioned in the report, however, are the unintended consequences of the actions taken by public health agencies across the country in 2020. The collateral damage of lockdowns included business closures, job losses, supply disruptions, mass protests, surging violence, increased mental health problems, unprecedented drug overdoses, and a collapse in cancer screenings. SENATE TESTIMONY: Child Suicide & Lethal Lockdown ConsequencesPublic health agencies, meanwhile, proved incapable of taming the coronavirus through the use of lockdowns. And these struggles were not confined to the United States.
The Lesson of LockdownsThe devastating impact of lockdowns, combined with their failure to slow the spread of the virus, demonstrates why states are right to curb the powers of public health agencies. If 2020 taught us anything, it’s the danger of unchecked executive power. Using emergency powers, governors and public health bureaucrats across the country took unilateral, sweeping, and indefinite measures that massively damaged livelihoods and infringed on the rights of millions of Americans. People were fined and arrested for simply gathering privately or exercising outside, walking a pet, paddling a boat on the water (alone), or taking a child to the park—even though most transmissions took place in homes and the coronavirus is rarely transmitted outdoors. Americans may disagree on the precise role public health departments should play in society today. But the pandemic reminded us why checks and balances on concentrated power are so important. The American constitutional system was deliberately designed to avoid concentrated power because the Framers feared it above all else.
The authors of the Network for Public Health Law report express concern that public health agencies are being stripped of the power to act by dangerous radicals. The truth is that dangerously radical government agencies are being put in check. Ohio, for example, passed a law in March that limits the length of a public health emergency order to 90 days unless it’s extended by the legislature. The same month, lawmakers in Utah passed legislation allowing the state legislature to override state health agency orders during public health emergencies. Missouri, meanwhile, has proposed a law that limits lockdowns to 15 days, after which extensions must be approved by legislative bodies. These reforms are not radical. They are both reasonable and sensible. They do not represent an attack on science—which tells us what is, not what we ought to do—but are prudent checks on power from lawmakers acting within their rightful province.
The preservation of liberty, protected by separating and checking power, is the ideal on which the American system was founded. Following a year that saw Americans’ rights, dreams, and health trampled by central planners wielding vast power with little restraint and few checks, it’s a vision Americans are right to rekindle. Just ask Mike Fratantuono and the millions of other Americans whose lives were derailed in 2020. |